Home, Search, Index, Links, Pathology, Molecules, Syndromes,
Muscle, NMJ, Nerve, Spinal, Ataxia, Antibody & Biopsy, Patient Info
|
Home, Search, Index, Links, Pathology, Molecules, Syndromes, Muscle, NMJ, Nerve, Spinal, Ataxia, Antibody & Biopsy, Patient Info |
|
Diagnoses to look for Pathology & Illustrations Indications & Utility Results: Differential diagnoses Technical (Preparation) Freezing Test form Skin biopsy Other Axons Myelin |
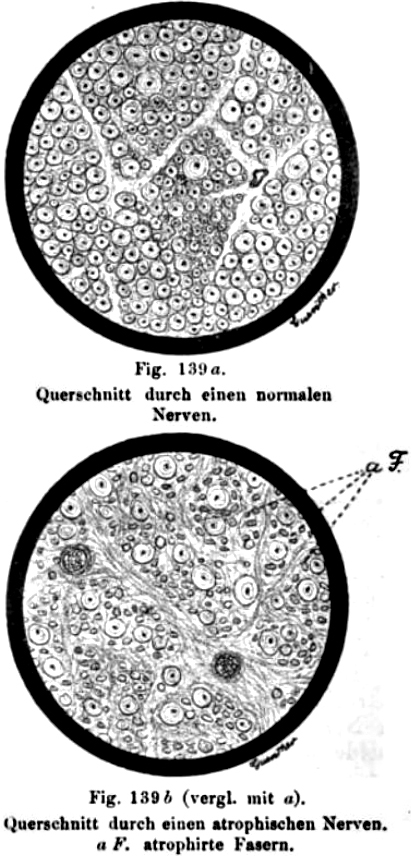
Nerve fascicle: Normal numbers of small and large axons
 NFH + Peripherin stain Myelinated axons: Surrounded by white halo Unmyelinated axons: Present in clusters between myelinated axons |

|
Useful biopsy results more likely
|
|
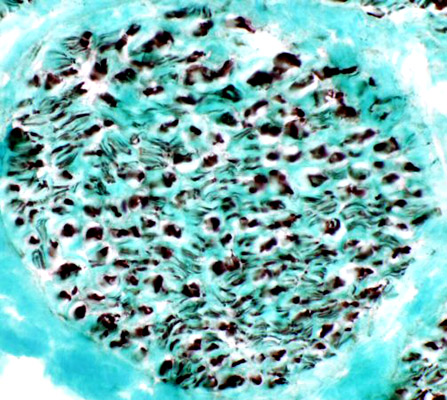
Neurofilament accumulations in neuropathy
|
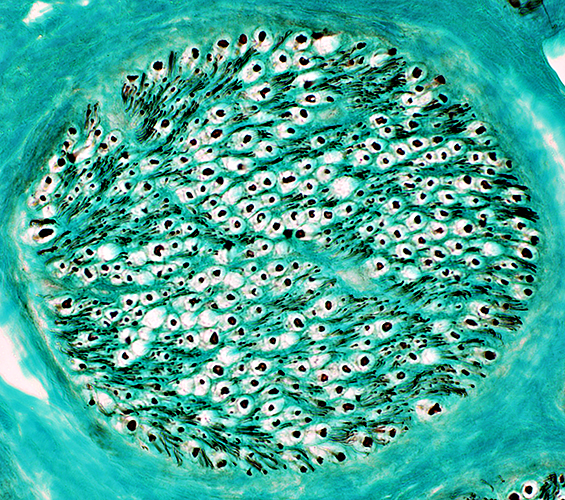
 SMI 31 antibody Sural nerve axons (Normal): Neurofilament stain
|