- Criteria
- Abdominal obesity (Waist circumference high)
- Males: ≥102 cm (≥ 40")
- Females: ≥88 cm (≥ 35")
- Atherogenic dyslipidemia
- Triglycerides: High; ≥ 1.7 mmol/l
- HDL cholesterol: Low
- Males: <1.03 mmol/l
- Females: <1.29 mmol/l
- Blood pressure: High
- Systolic: ≥130 mmHg
- Diastolic: ≥85 mmHg
- Insulin resistance
- Abnormal glucose testing: May occur as Type 2 diabetes
- May be associated with
- Dysregulation of fatty acid oxidation
- Increased myocellular lipid
- In untrained persons (non-athletes)
- Epidemiology
- Adult populations: 20% to 36%
- More with: Increased age (> 65 years)
- Females > Males
- Death ratio: Higher in males
- Children, Severely obese: 50%
- Associations
- Diabetes
- Control: Worse
- Disease duration: Longer
- Complications
- General: Nephropathy; Neuropathy
- Type 2: Cardiovascular Δ; Retinopathy
- Other
- Cardiovascular events
- Steatohepatitis, Non-alcoholic
- Deaths, Premature
- Non-essential amino acid (NEAA) metabolism: Disorders
- Serine & Glycine levels: Reduced
25
- L-serine deficiency in metabolic syndrome & diabetes
- Related to
- Impaired glycolysis
- Reduced synthesis of precursor: 3-phosphoglycerate
- Effects
- Phospholipid synthesis: Reduced and increased synthesis
- Deoxysphinganine synthesis: Increased
- Homocysteine disposal: Impaired
- Glycine: Deficiency
- Serine & Disorders
- Branched-chain amino acid (BCAA; valine, leucine, isoleucine) levels: High
25
- Contribute to
- Increased levels of aromatic amino acids (phenylalanine, tyrosine, tryptophan)
- Insulin resistance
- Adipokines: Leptin, Adiponectin, Resistin
- Predisposing factors
- Metabolic Syndrome in Obesity: Mitochondrial Dysfunction
- Subsarcolemmal mitochondria
- Generate ATP for energy requiring processes at cell surface
- Mitochondria may play role in propagation of insulin signaling
- Reduced oxidative enzyme capacity correlates with
- Severity of insulin resistance
- Reduced capacity for lipid oxidation
- Increased risk for obesity
- Subsarcolemmal mitochondrial electron transport chain activity is reduced in
- Obesity: 3.5 fold
- Type 2 diabetes: 7 fold
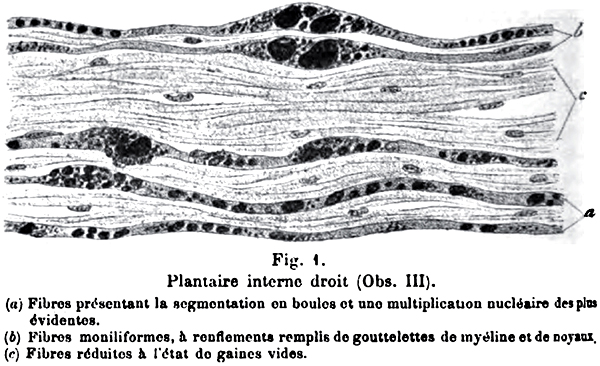
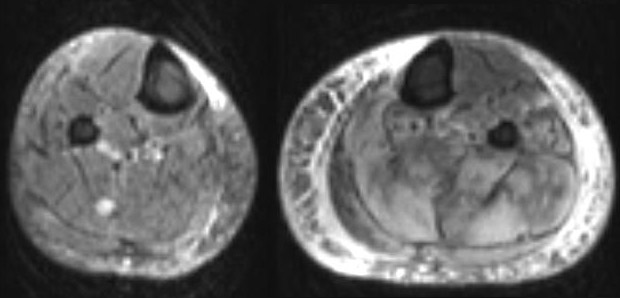
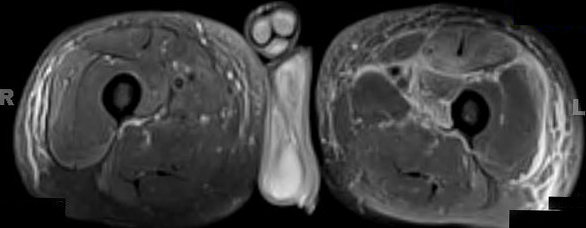
- Neuropathy in Obesity
26
|
| INTERPRETATION OF GLUCOSE TESTING |
| Glucose Pattern |
Fasting Glucose |
Glucose Load
(2 Hours after) |
| Normal |
< 100 mg/dl |
< 139 mg/dl |
| Impaired fasting |
100-125 mg/dl |
< 139 mg/dl |
| Impaired tolerance |
≤ 125 mg/dl |
140-199 mg/dl |
| Diabetes |
≥ 126 mg/dl |
≥ 200 mg/dl |
Fasting glucose: Overnight fast + Level drawn before 8:30 AM
Glucose tolerance: 75-g oral anhydrous dextrose load after fasting |
|