- Vitamin B12
- Cofactor for: Methionine synthase & l-Methylmalonylñcoenzyme A mutase
- Necessary for: Development & initial myelination of CNS
- DNA/RNA synthesis
- Daily requirement: 2.4 μg
- Forms
- Methylcobalamin
- Cofactor for: Methionine synthetase

- Converts
- 5-Methyltetrahydrofolate (5-MTHF) & Homocysteine to
- Products: Tetrahydrofolate & Methionine
- Methylcobalamin deficiency → ↑ Homocysteine →
- ↓ S-Adenosyl methionine → Impaired methylation reactions → Abnormal myelin
- Adenosylcobalamin
- Cofactor for: Methylmalonyl coenzyme A mutase (MMCoAM)
- Converts Methylmalonyl coenzyme A to Succinyl coenzyme A
- Methylcobalamin deficiency → ↑ Methylmalonic acid (MMA) →
- Abnormal fatty acid formation → Abnormal myelin structure
- Clinical features
- Polyneuropathy
- Symmetric
- Sensory change: 2° spinal or peripheral nerve lesions
- Early: Paresthesias
- Loss: Especially of large fiber modalities
- Distal
- Motor
- Distal weakness
- Later in disease course
- Reflexes
- Tendon: Reduced or absent at ankles
- Plantar: Upgoing
- Autonomic
- CNS
- Spinal cord: Earliest locus of involvement
- Major cause of sensory & motor disability
- Posterior column fiber loss
- Spasticity in legs
- Similar clinical features to N2O toxicity
- Other CNS
- Adults: Cognitive impairment
- Megaloblastic madness
- MRI: Leukoencephalopathy
- Childhood syndromes: Mental retardation or Encephalopathy
- Sensory
- Smell & Taste reduced
- Optic atrophy
- Gait ataxia
- Anemia: Due to reduced DNA synthesis
- Megaloblastic
- Hypersegmented neutrophils
- Leukopenia
- Thrombocytopenia
- LDH: High
- Haptoglobin level: Reduced
- Gastrointestinal: Glossitis; Diarrhea
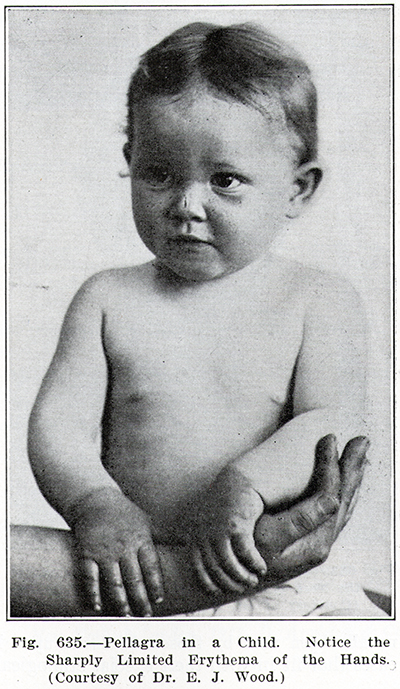
- Fingernails: Hyperpigmented
- Infants
- Development: Delay or Regression
- Hypotonia, Lethargy & Feeding difficulties
- Seizures
- Movements: Myoclonus; Choreoathetosis; Tremors
- Microcephaly
- Testing
13
- Serum: Presence of B12 deficiency
- B12 Low
- < 200 pg/ml
- 65ñ95% sensitive for proven clinical B12 deficiency
- 50% to 60% predictive of clinical response to B12 treatment
- Assay often unreliable: In presence of anti-intrinsic factor antibodies
- < 350 pg/ml
- Sensitivity: 90%
- Specificity: 25% for detecting high level of methylmalonic acid
- Homocysteine, Serum or Plasma, High

- Definition: Sum of
- Thiol-containing amino acid homocysteine +
- Homocysteinyl moiety of disulfides homocystine & cysteine-homocysteine: Free or bound to proteins
- Levels
- Normal < 14
- High > 15 μmol/L
- > 21 μmol/liter: 96% sensitive for clinical B12 deficiency
- B12 deficiency treatment: High homocysteine levels fall
- Homocysteine is elevated in serum in
- B12 deficiency
- Folate deficiency
- Renal insufficiency
- Diabetes
- Homocystinuria
: CBS (613381)
- N(5,10)-methylenetetrahydrofolate reductase deficiency
: MTHFR
- N2O
- Hyperhomocysteinemia in countries with folate-fortified food
- Associated disorders
- Atherosclerosis risk
- Recurrent arterial & venous thrombosis
- Neuropathy
- Lipid myopathy
- Lipid Myopathy with Hyperhomocysteinemia
27
- Clinical
- Onset age: 14 to 63 years
- Weakness (60%): Proximal; Legs
- Exercise intolerance
- Sensory loss: Pan-modal; Imbalance
- Laboratory
- Megaloblastic anemia (60%)
- Serum B12: Low
- Serum CK: 84 to 837
- EMG: Normal
- Muscle pathology: Lipid storage
- Methymalonic acid, Serum High (Normal < 400)
19
- Utility: Especially with B12 levels < 300 pmol/L
- > 400 nmol/liter: 98% sensitive for clinical B12 deficiency
- 300ñ1000 nmol/liter: Poor specificity for clinical response
- Megaloblastic anemia or Myelopathy: Levels of methylmalonic acid
- > 500 nmol per liter: Nearly all patients
- > 1000 nmol per liter: 86%
- False positive elevation of 300ñ700 nmol/liter
- Renal failure & Volume depletion
- B12 treatment: High levels fall
- Specific causes of B12 deficiency
- Pernicious anemia
- Intrinsic factor antibodies
- Sensitivity: 50%
- Specificity: 100%
- Must be tested > 7 days after vitamin B12 injection
- Prevents false positive result
- Parietal cell antibodies
- Sensitivity: 80%
- Specificity: 50% to 100%
- Rule out: Gastric cancer
- Atrophic body gastritis (Antral sparing; Autoimmune gastritis)
- Fasting high serum gastrin level (> 100 pmol/liter): Sensitivity 85%
- Pepsinogen I low in serum (< 30 μg/liter): Sensitivity 90%
- B12 malabsorption
- ? Increase serum holotranscobalamin level after oral loading: Not available in US
- Proven B12 deficiency in patient who eats meat or receives multivitamin therapy
- MRI: Hyperintense T2 spinal lesions
- Location: Posterior columns (50%)
- Lesions resolve after 8 to 12 months of therapy
- Evoked potentials
- Somatosensory: Abnormal tibial & median
- Motor: Normal in most
- Pathology
- Spinal cord
- Multifocal axonal loss & demyelination
- Localization
- Cervical & thoracic
- Posterior column > Anterolateral & Anterior
- Peripheral nerve: Axonal loss; Occasional ± demyelination
- Treatment
- Pernicious anemia: 1000 μg daily IM over 1 week; Then oral 1000 to 2000 μg daily for life
- Neurological involvement
- Alternate day hydroxycobalamin injections for 2 weeks
- Then normalize B12 levels
- Other malabsorption
- Oral cyanocobalamin 500 to 1000 μg daily for 1 week
- Taper to 1000 μg monthly
- Dietary deficiency: > 2 μg daily
- Infants: IM cyanocobalamin 250 to 1000 μg daily for 1 week; Then oral supplementation
- Oral & Parenteral administration may have similar efects to normalize B12
- Prognosis: Stabilization, or Some improvement
- Paresthesias
- Resolve within weeks
- Rarely transient exacerbation after treatment
- Myelopathy changes slowly if at all
- Causes of B12 deficiency: Normal body stores last 3 to 4 years
- Gastrointestinal malabsorption
- Deficient intrinsic factor production
- Post-gastrectomy
- Antibody vs parietal cells
6: Pernicious anemia
- Onset: Median = 60 years; Female slightly > Male
- Antibody targets: Gastric H+/K+-ATPase
- Catalytic α
subunit, and
- Glycoprotein β
subunit
- Regions of stomach affected: Fundus & body; Not antrum
- Mechanisms of B12 deficiency
- Reduced intrinsic factor production 2° parietal cell loss
- Antibodies to B12 binding site on intrinsic factor
- Prevent formation of complex normally carried to terminal ileum & absorbed
- Associated immune disorders
- Associated neoplasia: Gastric carcinoma (1% to 3%)
- Family history
- 20% of relatives also have pernicious anemia;
- Especially 1st degree females
- Gastritis treatment: Corticosteroids; Azathioprine
- No digestion of cobalamin-R-binder complex
- Consumption of cobalamin in GI tract
- Intestinal bacterial overgrowth
- Poor absorption by distal ileum
- Sprue-related disorders
- Autosomal recessive disorders
Anemia; Proteinuria; Juvenile onset
- Parasitic infection: Diphyllobothrium latum
- Dietary inadequacy in vegetarians
- Sources: Meat & dairy products
- Congenital disorders of B12 binding proteins
- Transcobolamin I (Vitamin B12 R-binding protein) deficiency
- Neurological B12 deficiency syndromes in adults
- Gastric intrinsic factor deficiency (IFD)
- Gene: GIF
- Congenital anemia & jaundice
- Transcobalamin II deficiency
- Gene: TCN2
- Megaloblastic anemia; Diarrhea; Immunodeficiency; Mental retardation
- Abnormalities of synthesis of active forms of B12
- Methylcobalamin deficiency
- Type E
: Methionine synthase reductase (MTRR)
- Type G
:
Methionine synthase (MTR)
- Neurological (CNS) & Hematological B12 deficiency syndromes
- Age: Children
- Methylmalonic aciduria, cblA type (Adenosylcobalamin deficiency)
- Gene: MMAA
- Episodic ketoacidosis; Encephalopathy; Neutropenia; Osteoporosis
- Combined methylcobalamin & adenosylcobalamin deficiency
- Methylmalonic aciduria & Homocystinuria, cblC type
: MMACHC
- Methylmalonic aciduria & Homocystinuria, cblD type
: MMADHC (C2orf25)
- Mental retardation; Anemia ± Myelopathy in slowly progressive cases
- Nitrous oxide exposure
- Oxidizes cobalt in cobolamin: Methylcobalamin inactivated
- Inhibits conversion of homocysteine to methionine:
- Reduced supply of S-adenosylmethionine (SAM)
- Abnormal release of B12 from lysosomes
- Methylmalonic aciduria & Homocystinuria, cblF type
: LMBRD1
- Methylmalonic aciduria & Homocystinuria, cblJ type: ABCD4
|
|
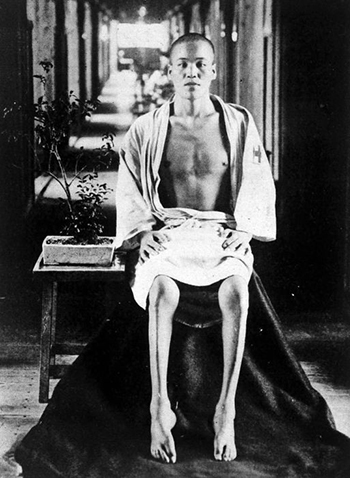
B12 deficiency: Spinal cord

Putnam
|
|