Home, Search, Index, Links, Pathology, Molecules, Syndromes,
Muscle, NMJ, Nerve, Spinal, Ataxia, Antibody & Biopsy, Patient Info
|
Home, Search, Index, Links, Pathology, Molecules, Syndromes, Muscle, NMJ, Nerve, Spinal, Ataxia, Antibody & Biopsy, Patient Info |
|
Causes Adult onset Infantile onset Evaluation & Management Exacerbating factors Home ventilation Spirometric abnormalities |
|
|
||||||||||||||||||
|
Restrictive ventilatory defects are characterized by proportional
decreases in FVC and FEV1, leaving the FEV1/FVC
normal or even slightly elevated. Any lesion affecting the lung, chest
wall, or respiratory muscles that reduces the ability to take in a normal amount of
air but does not affect the conducting airways is classified
as a restrictive lung disease. |
||||||||||||||||||
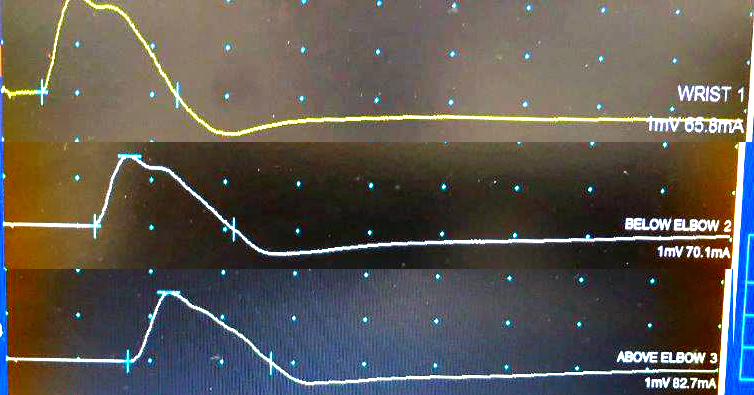 From: M. Al-Lozi CMAPs: Slow & Prolonged Repolarization
|
