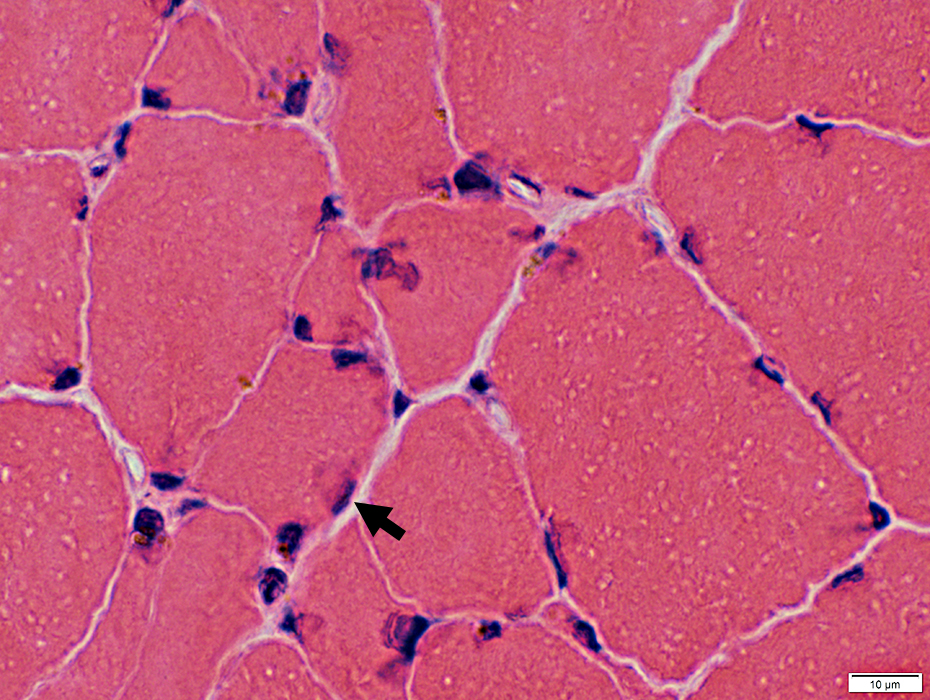
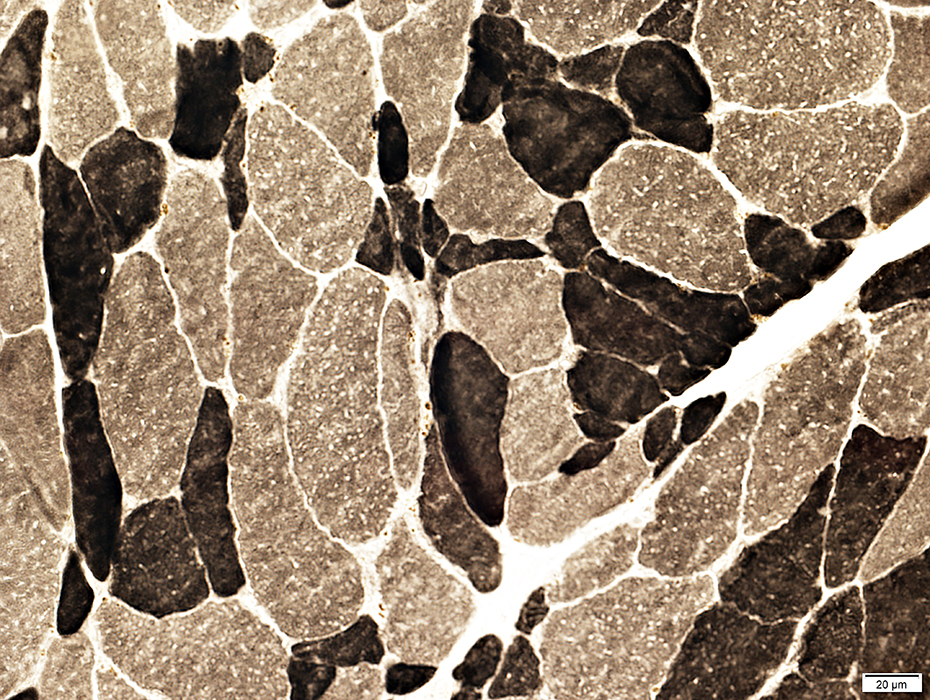
Cachexia
3
- Definitions
- Sarcopenia + Weight loss + Low BMI
- Wasting of Skeletal muscle ± Fat despite nutrition support
- Disease-related malnutrition with systemic inflammation
- Quantitative
- Weight loss ≥
- 5% within 6 months
- 2% + Body mass index (BMI) <20 kg/M2
- 2% + Sarcopenia
- Laboratory
- C-reactive protein (CRP): > 1.0 mg/dL
- Albumin: < 3.5 g/dL
Common with
- Advanced cancer: Accounts for 30% of deaths
Effects
- Morbidity: Increased and reduces both
- Tolerance & Responsiveness to treatment: Reduced
Cancer Cachexia: Associated with
- Bone morphogenetic protein (BMP) signaling: Reduced
4
- Expression of Noggin (BMP inhibitor) increased in muscle
- Triggered by
- Activin A (IHNBA)

- IL-6
- Cancer-mediated factors
- Proteolysis-inducing factor (PIF; Dermicidin; CCF1)
- Lipid-mobilizing factor (LMF; ZAG)
- TNF-α
- Parathyroid Hormone-like protein (PTHRP; PTHLP)
- Adipose wasting: UCP1
- Anorexia & CNS
- Proopiomelanocortin (POMC)
- Cart Prepropeptide (CART; CARTPT)
|
|
Cachexia |
Starvation |
| Body Weight |
↓ |
↓ |
Skeletal
Muscle |
↓ |
→ |
Adipose
Tissue |
↓ |
↓ |
Rest Energy
Expenditure |
↑ |
↓ |
Inflammatory
Markers |
↑ |
→ |
|