- Length: Mean = 15.3 cm
- Regions
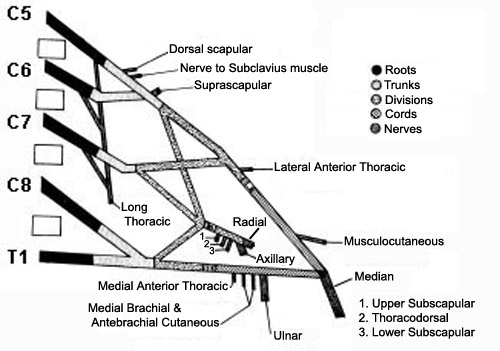
- Roots
- Number
- Usual: 5; C5 to T1
- Variants
- C4 & T2 may contribute axons to plexus
- No effect on lesion location
- Most proximal areas of plexus
- Root branches to brachial plexus: Anterior primary rami
- Located deep in neck: Between anterior & middle scalene muscles
- Nerves directly from anterior primary rami
- Scalene muscles (C5 - C8)
- Longus coli (C5 - C8)
- Long thoracic nerve to serratus anterior (C5 - C7)
- Phrenic nerve, inferior contribution (C5)
- Dorsal scapular to rhomboids & Levator scapulae (C5)
- No somatic axons originate from T1 anterior primary rami
- Most motor axons: C5 & C6
- Most sensory axons: C7
- Trunks
- Number: 3; Upper, Middle, & Lower
- Location
- Posterior cervical triangle
- Behind clavicle & sternocleidomastoid muscle
- Lower trunk: Adjacent to subclavian artery & apex of lung
- Divisions
- Number: 6; 3 Anterior & 3 Posterior
- Location: All retroclavicular
- Functions
- Anterior divisions: Tend to supply flexor muscles
- Posterior divisions: Tend to supply extensor muscles
- Cords
- Number: 3; Lateral, Posterior & Medial
- Location: Near axillary artery & lymph nodes; Below pectoralis minor
- Terminal nerves
- Location of origin: Distal axilla
- Anatomical classification of lesions
- Supraclavicular
- Anatomy: Root & Trunk lesions
- Frequency: More common
- More frequently due to closed traction
- More severe
- Myelogram: Root avulsion
- Deformed dural pouches
- Poor root sleeve filling
- Cord edema or atrophy
- Most reliable for C8 & T1 lesions
- Outcome
- Generally worse
- Upper lesions: Best prognosis
- More commonly demyelinating
- Closer to innervated muscles
- Surgically accessible
- Specific syndromes
- Retroclavicular
- Anatomy: Divisions
- Usually associated with upper or lower plexus lesions
- Isolated lesions: Uncommon
- Infraclavicular
- Anatomy: Cords & Terminal nerves
- No regional differences in incidence, severity, prognosis
- Associated lesions: Humeral fracture; Glenohumeral dislocation
- Electrophysiology of brachial plexus lesions
- Useful for differentiating pre- & post-ganglionic lesions
- SNAPs: Useful for localization of root lesions
- CMAPs: Useful for determining
- Demyelination
- Severity of lesions (before reinnervation)
|
|
|
Muscle Innervation: Brachial Plexus
|
Trunks
Upper trunk (C5-C6)
Supraspinatus
Infraspinatus
Biceps
Deltoid
Teres minor
Triceps
Pronator teres
Flexor carpi radialis
Brachioradialis
Extensor carpi radialis
Brachialis
Middle trunk (C7)
Pronator teres
Flexor carpi radialis
Triceps
Anconeus
Extensor carpi radialis
Extensor digitorum communis
Lower trunk (C8-T1)
Abductor pollicis brevis
Flexor pollicis longus
Pronator quadratus
Extensor indicis proprius
Extensor pollicis brevis
Extensor carpi ulnaris
First dorsal interosseous
Abductor digiti minimi
Adductor pollicis
Flexor digitorum profundus
Flexor carpi ulnaris
|
Cords
Lateral cord
General: Musculocutaneous & Median
Biceps
Brachialis
Pronator teres
Flexor carpi radialis
Medial cord
General: Median & Ulnar nerves
Abductor pollicis brevis
Opponens pollicis
Flexor pollicis longus
First dorsal interosseous
Adductor pollicis
Abductor digiti minimi
Flexor carpi ulnaris
Flexor digitorum profundus
Posterior cord
General: Axillary & Radial nerves
Latissimus dorsi
Deltoid
Teres minor
Triceps
Anconeus
Brachioradialis
Extensor carpi radialis
Extensor digitorum communis
Extensor pollicis brevis
Extensor carpi ulnaris
Extensor indicis proprius
|
|