Thymoma
- Thymoma: General
- Definition: Neoplasm of epithelial cells of thymus
- Location
- Anterior mediastinum: 90%
- Most common anterior mediastinal mass in adults (20% to 50%)
- Age
- Most common in 4th to 6th decades
- Uncommon: Children; MG onset > 65 years
- Male = Female
- Prognostic features
- Invasive (35%): Poorer prognosis
- Non-Invasive (Encapsulated; 65%): Better prognosis
- Thymic carcinoma: Poor prognosis
- Treatments
- Stage 1 (Encapsulated)
- Stage 2 (Macroscopic invasion into capsule, fat or pleura)
- Tumor resection
- Then Irradiation
- Stage 3 (Macroscopic invasion into neighboring organs)
- Neoadjuvant Chemotherapy
- Tumor resection
- Irradiation
- Consolidation Chemotherapy
- Thymoma: Associated Paraneoplastic syndromes (PNS)
23
- General
- 50% of thymomas present with paraneoplastic syndrome
- 33% of thymoma PNS have > 1 disorder
- Onset: Before, or After, thymoma treatment
- Thymoma survival: Better if PNS resolves
- Neuromuscular
- CNS
- Hematologic
- Pure red cell aplasia: 5% to 8% of Thymomas
- Hypogammaglobulinemia (Good syndrome)
- Acquired
- Frequency: 3% to 6% of Thymomas
- Associations: Adult-onset immunodeficiency
- B cells: Low or absent
- Defects in cell-mediated immunity
- Inverted CD4/CD8(+) T-cell ratio
- Infections: CMV
- Lymphocytosis
- Myocarditis
- Skin
- Alopecia/Vitiligo
- Pemphigus
- Lichen planus
- Candida
- GI: Pseudo-obstruction
- Antibody vs 66 kDa rat brain antigen (CV2)
- Rx pyridostigmine
- Endocrine
- Hypercalcemia
- Cushing syndrome
- Other immune
- Thymoma: Associated autoantibodies
9
- Anti-AChR antibody (Binding) association
- Patients with MG and thymoma: Frequency = 95% to 100%
- Thymoma without clinical MG
- Other associated neurological disorders: 50%
- No associated neurologic disorders: 30%
- Striational
- Titin
- Common: Thymoma+MG & Late onset MG
- Uncommon: Young-onset MG
- Ryanodine receptor
- Thymoma + MG > Thymoma- MG
- Cytokines: IL12, INFα
- Titin: Common in Thymoma-MG & Late onset MG
- KCNA4
- Glutamic acid decarboxylase
- Frequency: 22%
- Higher with associated neurological syndromes
- Hu (Antineuronal nuclear antibody-type 1 (ANNA-1))
- CASPR2
- DCC
- Lgi1
- Thymoma types: Lymphoepithelial
- Noninvasive thymoma
- Almost all are > 25 years old
- Most common: 5th to 6th decade
- Calcification in 5-20%
- Invasive thymoma
- Metastasis to pleura and lungs (6%); rarely extrathoracic
- Thymic tumors & Myasthenia gravis
35
- Frequency
- MG: Most common thymoma paraneoplastic syndrome
- MG in 20% to 40% of Thymomas
- Serum Nicotinic AChR antibodies
15
- MG + Thymoma: (99%)
- Thymoma without symptomatic MG: 30%
- Thymoma in MG
- 7% to 15% of MG patients
- Mostly in MG patients > 30 years
- MG: Frequency varies with thymoma type
- Thymomas + MG: Usually composed of cortical cells
- Other thymomas
- Mixed pattern
- More undifferentiated malignancy
- Tumor type relations
| Tumor |
Spread |
MG
frequency |
| A: Medullary (Spindle cell) |
- |
+ (17%) |
| AB: Mixed |
- |
++ (18%) |
| B1: Lymphocyte-rich |
++ |
+++ (44%) |
| B2: Cortical |
++ |
+++ (54%) |
| B3: Well differentiated (Squamoid) |
+++ |
+++ (50%) |
| Thymic carcinoma |
+++ |
- |
- Myasthenia gravis + Thymoma: Clinical
25
- General: Similar to other AChR-Ab+ MG
- Differences vs other AChR-Ab+ MG: May be
- More Generalized
- More Severe
- Difficult to treat
- Worse prognosis
- May be associated with: Other paraneoplastic disorders
- Thymoma recurrence
- May be associated with MG worsening
- Risk: Dependent on thymoma pathological stage
- Non-resectable thymoma: MG may be more severe
- No HLA association identified
- MG Prognosis better
24
- AChR antibody: Positive
- Thymic follicular hyperplasia
- Non-recurent neoplasm
- No relation to tymoma tissue subtype
- Muscle pathology: Increased frequency of lymphorrhages
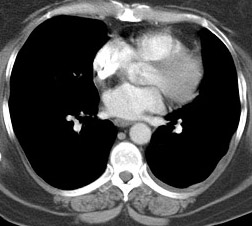
- Clinical work-up
- Computed tomography scan of the thorax
- Modality of choice
- Contrast-enhanced: If thymomas suspected; Greater diagnostic yield
- Performed to look for thymoma in MG patients aged ≥ 20 years
- MRI examinations of the chest
- More expensive
- Not clearly superior
- Utility: Iodine allergy; Renal failure
- Thymoma features
- T1 signal: Intermediate
- T2: Heterogeneity & Variable enhancement
- High-risk lesions: More heterogeneous
- Therapeutic implications
- Removal of thymoma
- General: Trans-sternal approach
- Early stage thymoma: Minimally invasive surgery
- MG
- ? More difficult to manage after thymoma removed
- New MG: May appear after thymectomy: ? more in AChR Ab+ patients
|

Bell 1917
|
|