A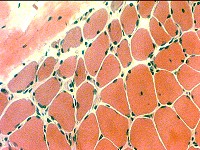 H & E stain |
Describe the pattern of abnormality of muscle fibers. Answer: Perifascicular atrophy of muscle fibers What other structure is commonly damaged in these regions? Answer: Capillaries are damaged and lose their endothelium. What is the most likely diagnosis? Answer: Dermatomyositis with vascular pathology This is the typical pathology seen in children, and some adults, with dermatomyositis. There is muscle fiber atrophy and vacuolarization but little necrosis It differs from another type of dermatomyositis (IMPP) that has Damaged perimysium with histiocytic (Acid phosphatase-positive) cellularity No capillary pathology. Strong associations with: Interstitial lung disease; tRNA synthetase antibodies |
B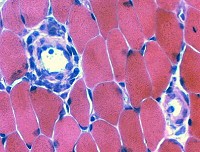 H & E stain |
How would you interpret this finding? Answer: Mononuclear cell infiltrate around an intermdiate-sized blood vessel The perivascular infiltrate is suggestive of an immune disorder. There is no damage to the vessel wall that would suggest a vasculitis. There are no myopathic changes to support a diagnosis of myositis. |
C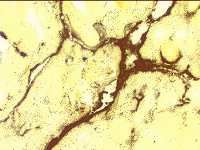 Alkaline phosphatase stain |
Alkaline phosphatase diffusely stains the perimysium in this low power image of a muscle. How would you interpret this pattern of abnormality? Answer: Alkaline phosphatase staining of perimysium supports a diagnosis of an immune mediated, often treatable, myopathy What other patterns of abnormal alkaline phosphatase staining occur in muscle? Answer: Alkaline phosphatase staining Around the rim of muscle fibers: Muscle fiber necrosis Capillaries near regions of perifascicular atrophy: Common in childhood dermatomyositis Muscle fiber cytoplasm: Immature or regenerating muscle fibers |
D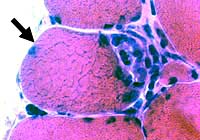 H & E stain |
What is wrong with the muscle fiber? Answer: Focal invasion of muscle fiber by inflammatory cells How would you interpret this finding (focal invasion)? Answer Focal invasion of muscle fibers can occur in both Polymyositis and Inclusion body myositis. The finding does not distinguish between treatable myositis and untreatable IBM-like disorders What other stains might be performed to clarify the disease process? Answer Cells invading muscle fibers are commonly labeled by: Acid phosphatase and Non-specific esterase. Evaluation for IBM-like disorders: Congo red for vacuoles; SMI-31 for aggregates |
E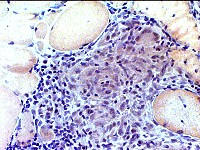 Congo red stain |
What does this pattern of focal cellularity suggest? Answer: Granuloma There are multinucleated giant cells What additional stains would be useful to confirm your impression? Answer: Esterase and Acid phosphatase will stain most of the histiocytic cells in the center of granulomas Giant cell markers are: Lysozyme; α1-antichymotrypsin Small dark cells surrounding the histiocytic cells, and often extending into the endomysium. are lymphocytes. |
F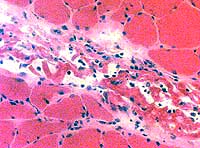 H&E stain |
What does this pattern of pathology suggest? Answer: Perimysial damage, Often immune-mediated What additional stains would be useful to confirm your impression? Answer: Perimysial cellularity often stain with Esterase and Acid phosphatase. What is a differential diagnosis for this pattern of pathology? Answer: Acid phosphatase-positive cellularity in the perimysium commonly occurs in Fasciitis (Immune or Toxic). Immune myopathies with perimysial pathology (IMPP) IMPP syndromes are multisystem disorders. Other systems often involved include skin (Dermatomyositis subtype) and lungs (Interstitial lung disease). Graft-vs-Host Disease |
G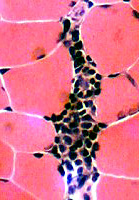 H&E stain |
47 year old female with recent onset bulbar and proximal arm weakness and normal serum CK. What does this pattern of inflammation suggest? Answer: The dark mononuclear cells are probably lymphocytes forming a lymphorrhage. What additional tests would be useful to confirm your impression? Answer: Repetitive nerve stimulation; Anti-AChR antibodies; Chest CT Esterase stain showed small, multifocal neuromuscular junctions. The patient had myasthenia gravis and thymoma. |