A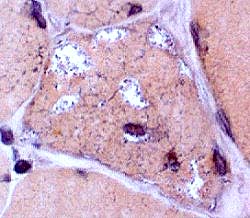
|
A 64 year old female complains of difficulty swallowing and arising from chairs. Examination shows asymmetric patchy weakness, especially in the quadriceps and hand grip. Serum CK is 300. Image: Congo red stain highlights irregular vaculoes Answers: MHC Class I: Upregulated in sIBM but not hereditary disorders SMI-31: Shows aggregates in muscle fibers Lymphocyte stains: Shows inflammation in sIBM but not hereditary disorders Likely diagnosis: Inclusion body myositis Differential diagnosis of vacuoles with basophilic debris in muscle fibers: Distal myopathies; HIBM2; Oculopharyngeal dystrophy |
B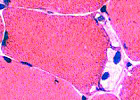
|
A 20 year old male noted muscle discomfort during intense exercise. Examination shows normal strength, and a tendency to "give way". Serum CK is 500. EMG is myopathic. Image: H&E stain shows subsarcolemmal blebs. Some contain nuclei Answers: PAS: Increased in muscle fibers in some patients. Phosphorylase: Absent in most muscle fibers; Present in vessels & regenerating fibers Diagnosis: Phosphorylase deficiency (McArdle's) |
C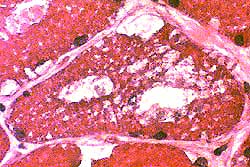
|
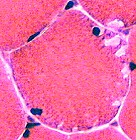
A 35 year old male is admitted to the ICU for respiratory failure. Exam shows a vital capacity of 50% of predicted, and weakness of thigh adductors. Serum CK is 1,465. EMG shows myopathy and fibrillations. Image: H&E stain shows cytoplasmic & subsarcolemmal vacuoles. Answers: PAS: Increased in muscle fibers in children Acid phosphatase: Positive staining granules in muscle fiber cytoplasm Biochemical analysis for Acid maltase activity in muscle & blood Diagnosis: Acid maltase deficiency |
D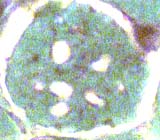
|
An 8 year old female has chronic, slowly progressive weakness. She was normal until 1.5 years of age. Examination shows weakness in proximal & facial muscles. Serum CK is 600. Cardiac evaluation: Ventricular hypertrophy & R bundle branch block. Image: Gomori trichrome shows multiple clear round regions in muscle fiber cytoplasm Answer: Sudan Black, or Oil Red O, stains lipid in muscle fibers Diagnosis: Lipid storage, often Carnitine disorders |
E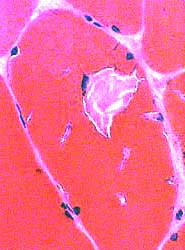
|
An 20 year old male is evaluated for myalgias. Examination shows mild proximal weakness. Serum CK is 300. Answer: NADH stains tubular aggregates dark Morphologic diagnosis: Tubular aggregates NOTE: Tubular aggregates are not a final diagnosis and can occur in many disorders. They are common in: Hypokalemic periodic paralysis |
F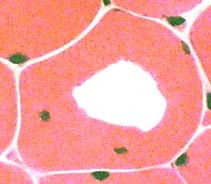
|
A 20 year old male has frequent episodes of weakness on awakening. Now he is having difficulty arising from chairs. Examination shows mild proximal weakness. EMG is myopathic. Image: H&E stain shows a clear region within scattered muscle fibers. Answer: H&E evaluation of other muscle fibers Diagnosis: Hypokalemic periodic paralysis Differential diagnosis: Freeze artefact (Change would be present in many contiguous, not scattered, fibers) |