General
- Epidemiology: Varied frequency
- 1.9 per 100,000 in Japan
- 8.4 per 100,000 in Western countries
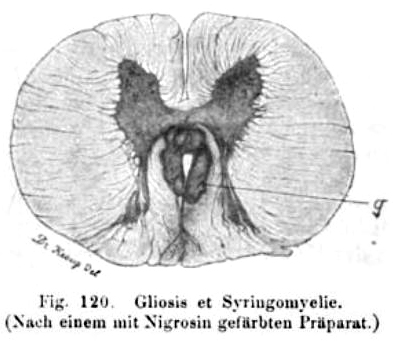
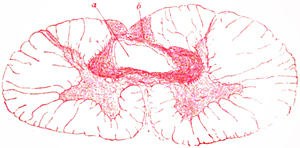
- Pathology
- Cavitation: Fluid filled
- Surrounding tissue: Gliosis
- Location
- Spinal cord
- Usually cervical or thoracic: C2 to T9
- Medulla
- Course: Chronic
- Children: Usually occurs with congenital anomalies
- Adults
- Onset: Most commonly between ages 25 to 40
- Males > Females
- Causes
- Prior events: Meningitis; Spinal trauma
- Neoplasms: Intramedullary or Extramedullary
Syndromes & Features
- Clinical features: Variable depending on anatomical involvement
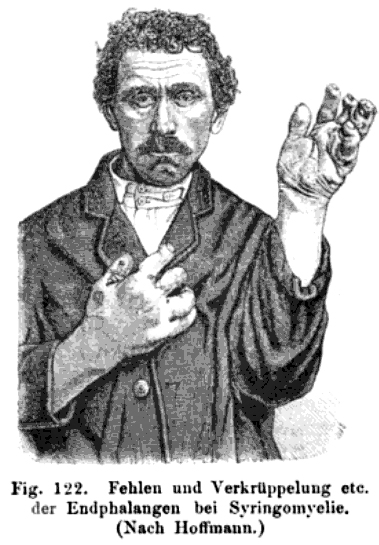
- Anterior horns
- Weakness & Wasting: Especially in hands & arms
- Fasciculations
- Posterior horns & Decussating sensory fibers
- Sensory loss: Pain & Temperature
- Distribution: "Suspended" sensory loss
- Involves: Arms & Trunk
- Spares: Legs
- Sacral Involvement: May suggest neoplasm
- Pain: Occasional; Boring or lancinating
- Large fiber sensations: Usually preserved
- Tendon reflexes: Reduced or absent in arms
- Autonomic pathways
- Horner's syndrome
- Skin: Trophic changes
- Neurogenic bladder: Late in disease course
- Corticospinal tracts: Variable involvement
- Spastic paraparesis: Legs > Arms
- Skeletal
- Cranial nerve involvement: With syringobulbia
- Most often unilateral
- XII: Tongue weakness & hemiatrophy
- IX - X: Dysphagia; Dysarthria
- XI: Weakness & wasting of sternomastoid & trapezius
- VII: Facial paresis
- Descending tract of V
- Reduced pain & temperature on lateral face
- "Onion skin" distribution
- Reduced corneal sensation & reflex
- Course: Very slow progression
- Surgical treatment: Posterior fossa decompression
1
- Variant syndrome: Neural tube defects
- Distribution: Legs
- Weakness
- Bowel & Bladder dysfunction
- Pain
- Association: Chiari II malformation
- Variant syndrome: Presyrinx
2
- Spinal cord edema
- Caused by alterations in CSF flow at foramen magnum
- Location: Cervical or Thoracic
- Associated with disorders that disrupt CSF flow
- Chiari I & II malformations
- Trauma
- Subarachnoid hemorrhage
- Bacterial meningitis
- Cervical stenosis
- Posterior fossa arachnoid cyst
- Spinal arachnoiditis
- Neurosarcoidosis
- Clinical
- Onset age
- General: 1 year to Adult
- Chiari malformation: Childhood
- Course
- Onset may be acute or subacute
- Some with chronic progression
- MRI change may be asymptomatic
- Weakness: Arms or Quadriparesis
- Headache
- Bulbar: Dysphagia & Gagging
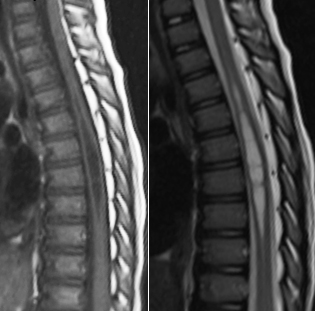
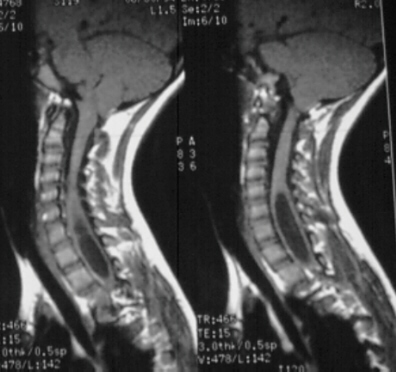
- MRI
- T2 prolongation
- T1 prolongation
- Cord enlargement without enhancement
- Treatment: Reversible with surgery
- Animals: Syrinx & Arnold-Chiari predisposition
- Cavalier King Charles Spaniel
- Brussels Griffon
Syrinx: Associated disorders
- Childhood forms: General
- Embryonic
- Central canal of spinal cord: Abnormal dilatation
- Roof plate: Thin & Elongated
- Mesenchymal tissue
- Reduced between spinal cord & surface ectoderm
- Neural tube defect
- Open
- Gap in posterior vertebral arches
- Meneingomyelocele: Extensive syrinx to cervical levels
- Fetal
- Mesenchymal tissue: Normal
- Neural tube defect: Closed; Intact vertebral column
- Syrinx
- Located rostral to tethering lipoma or bony spur
- Stays localized to lower thoracic & lumbar levels
- Specific causes
- Later onset
- Prior event: Trauma; Hematomyelia; Meningitis
- Neoplasms
- Intrinsic
- Spinal cord glioma
- Ependymoma
- Hemangioblastoma
- Extramedullary: Tumors; Arachnoid cysts
- Spinal canal stenosis
- ? Cervical rib
- Radiology: A;
B
|
|


{kind=link}