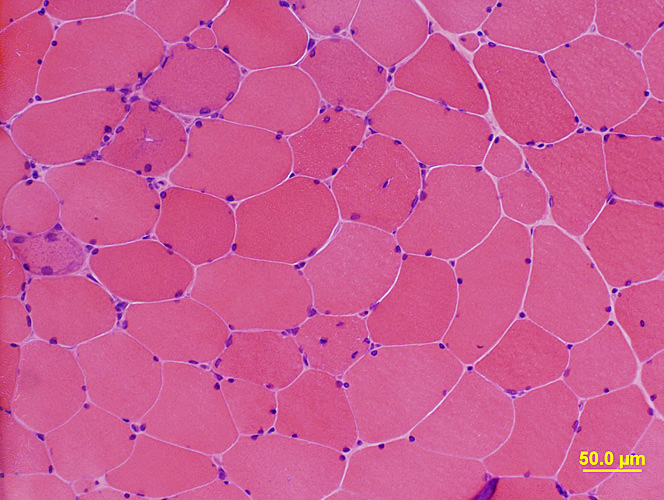
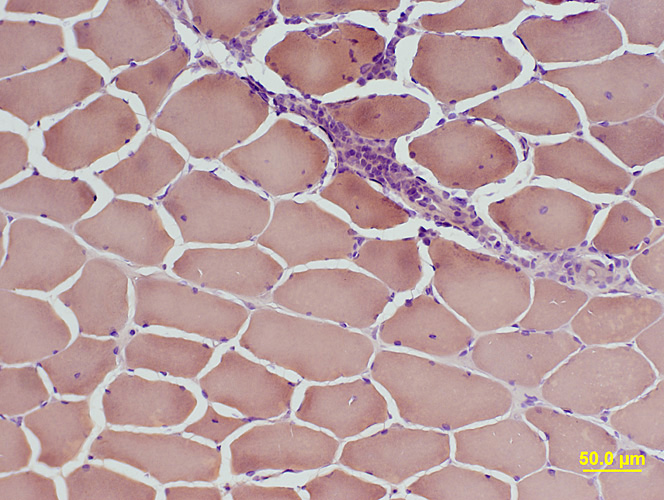
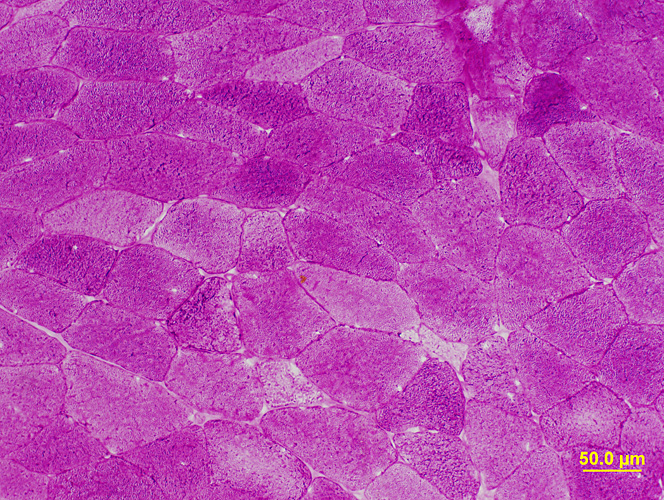
 H&E stain |
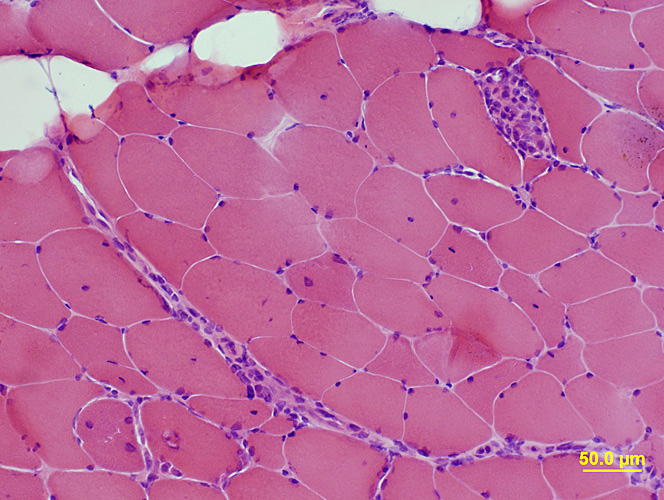 H&E stain |
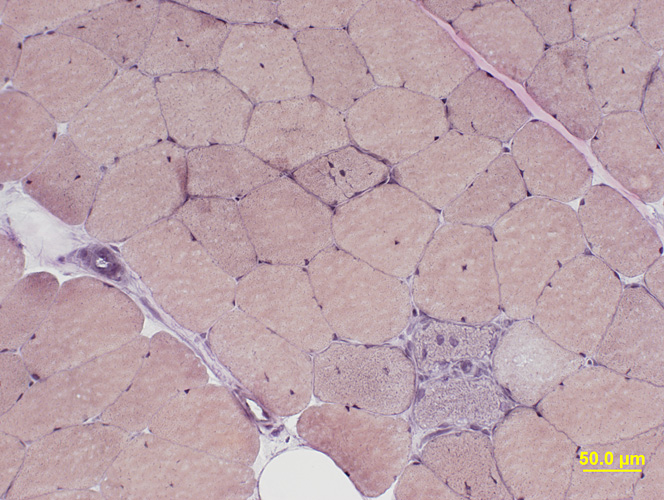
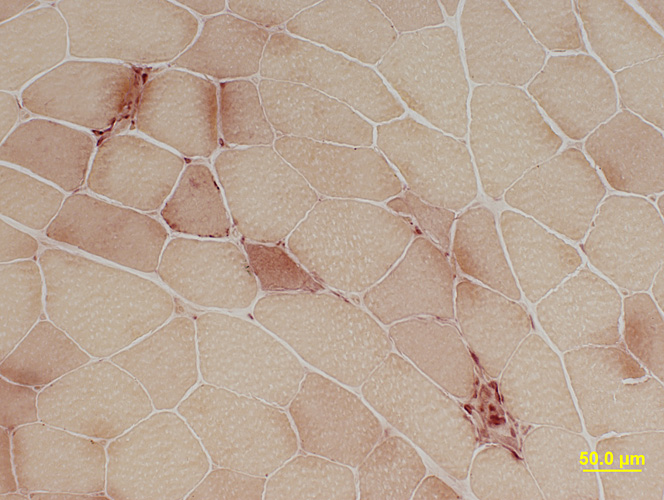
 Gomori Trichrome stain |
 VvG stain |
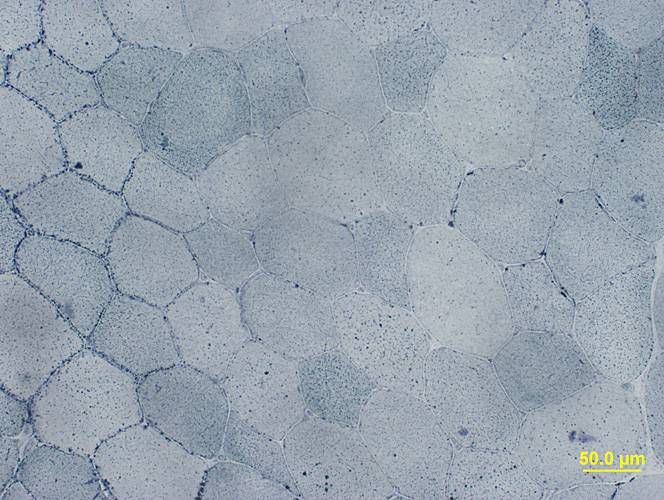
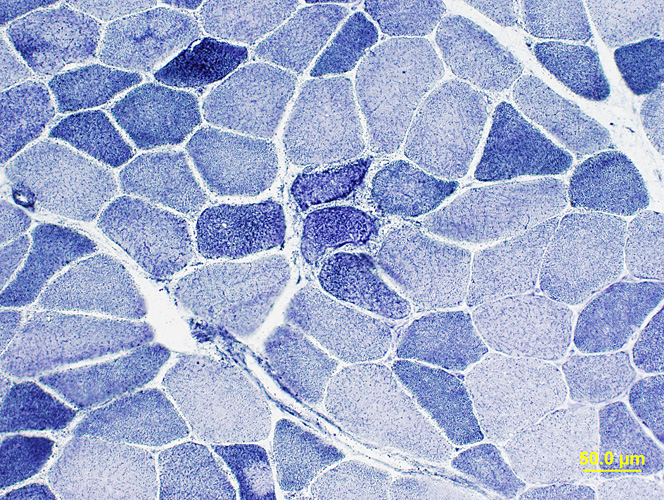 NADH stain |
 Congo Red stain |
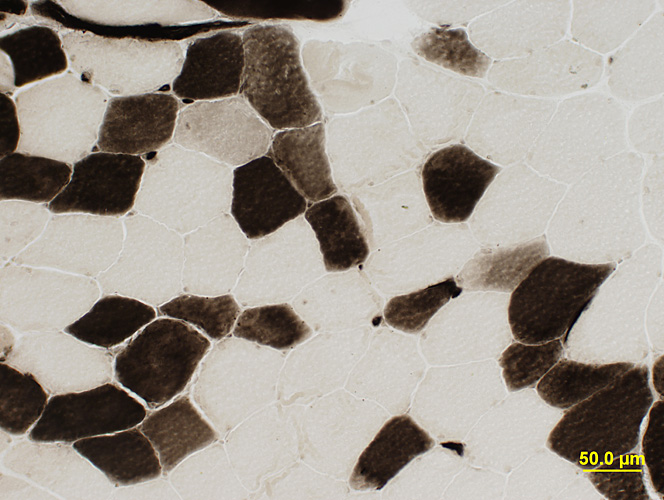
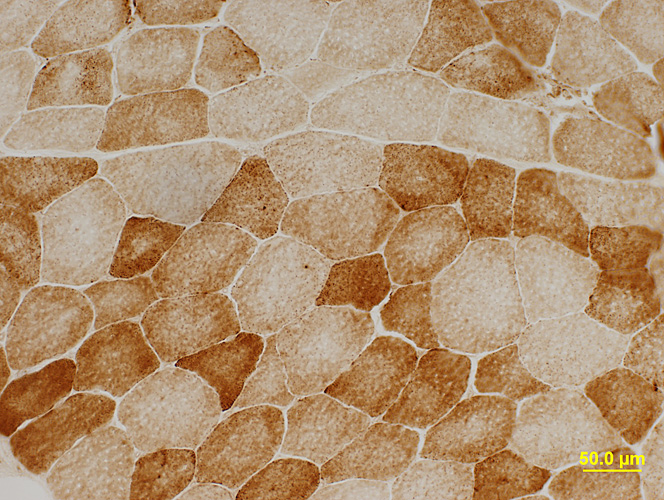
 ATPase pH 9.4 stain |
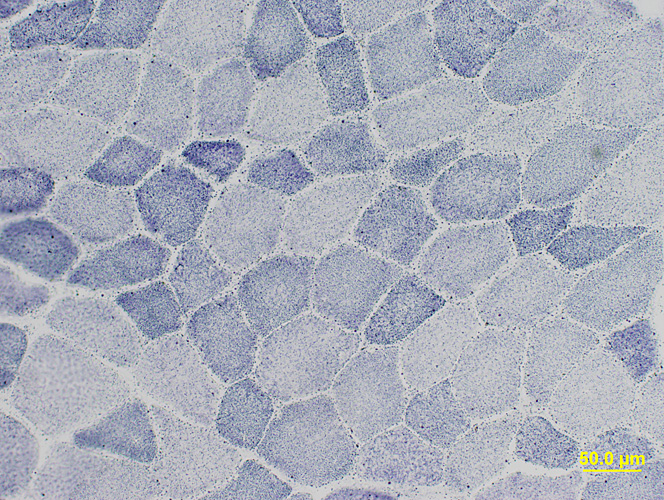
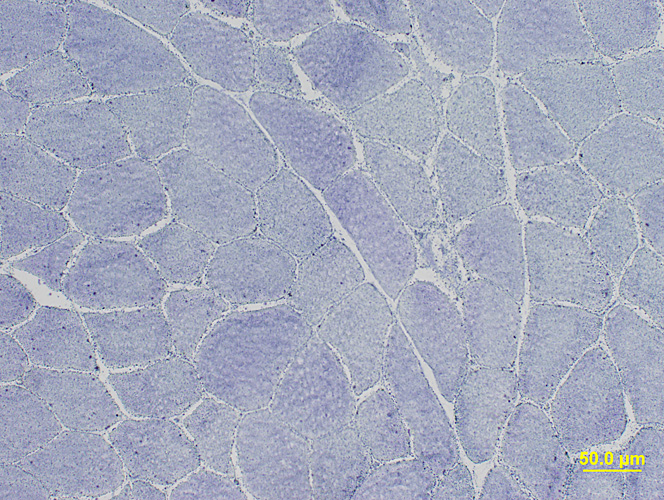
 ATPase pH 4.3 stain |
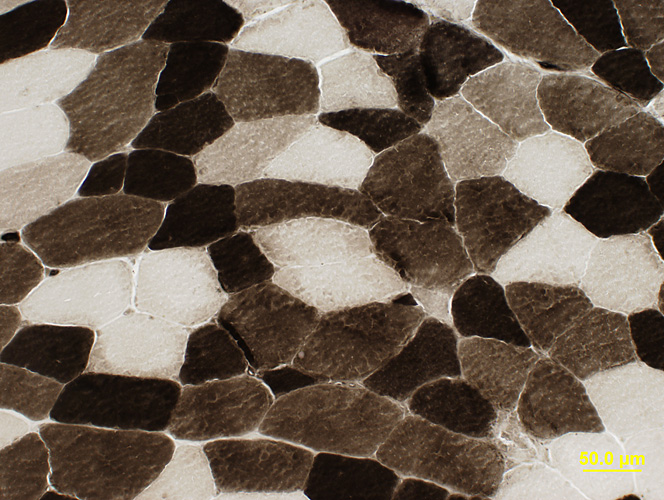 ATPase pH 4.6 stain |
 Alkaline Phosphatase stain |
 Acid Phosphatase stain |
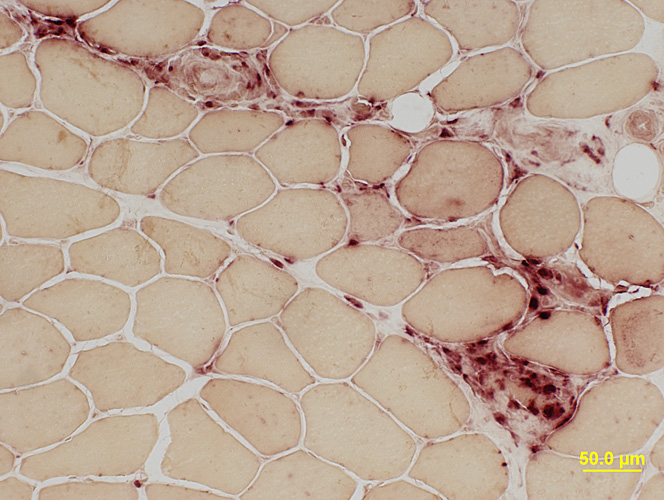 Acid Phosphatase stain |
 Esterase stain |
 Sudan Black stain |
 PAS stain |
 Succinate Dehydrogenase (SDH) stain |
 Cytochrome Oxidase (COX) stain |
 Phosphorylase stain |
 AMPDA stain |
|
BIOPSY REPORT Clinical history: 47-year-old female with weakness and pain Description of Muscle (Microscopic; Sections of snap frozen muscle): H&E stain shows scattered necrotic and basophilic muscle fibers. Endomysium shows mildly increased regional cellularity. Endomysial connective tissue is normal. A smaller perimysial vessel is associated with inflammatory cellularity. There are no distinctive morphologic abnormalities on Gomori trichrome or VvG. NADH shows scattered dark, or coarse, staining smaller muscle fibers. Congo red highlights one or two regions of perimysial cellularity. Alkaline phosphatase is unremarkable. Esterase highlights occasional small muscle fibers with dark staining and a necrotic fiber. Acid phosphatase highlights perimysial cellularity, cells associated with necrotic muscle fibers, and cells near muscle fibers that appear to be focally invaded. COX and SDH show no mitochondrial pathology. There is no storage material on PAS or Sudan. AMPDA and phosphorylase are present. ATPase (pH 9.4, 4.6 and 4.3) shows no muscle fiber type grouping. There are scattered type IIC muscle fibers on ATPase pH 4.3. ATPase pH 4.6 shows varied degrees of intermediate staining in some fibers. Interpretation: Abnormal muscle biopsy with mildly active myopathic changes and scattered endomysial and perimysial inflammation. Inflammation in the perimysial connective tissue is acid phosphatase positive. This pattern of abnormalities suggests an immune, inflammatory myopathy. Immune stains will be performed to further characterize the inflammatory and immune process. Myositis-specific antibodies may be of use for further diagnostic classification. |