Immune Myopathy with Antibodies to Signal Recognition Particle
|
SRP pathology Early Intermediate Late, Severe Late, Mild Capillaries Complement deposition |
General features
- Muscle fibers: Myopathy, ongoing
- Active: Necrosis & Regeneration; Early in course
- Fiber size: Varied (Bimodal)
- Many immature (Type 2C) fibers
- Connective tissue
- Endomysial: Increased early & late in disease course
- Basal lamina: Thickened
- Endomysial capillaries: Reduced number; Enlarged; C5b-9 deposition
- Immune
- Inflammation: Little or none
- MHC Class I: Often normal on muscle fibers
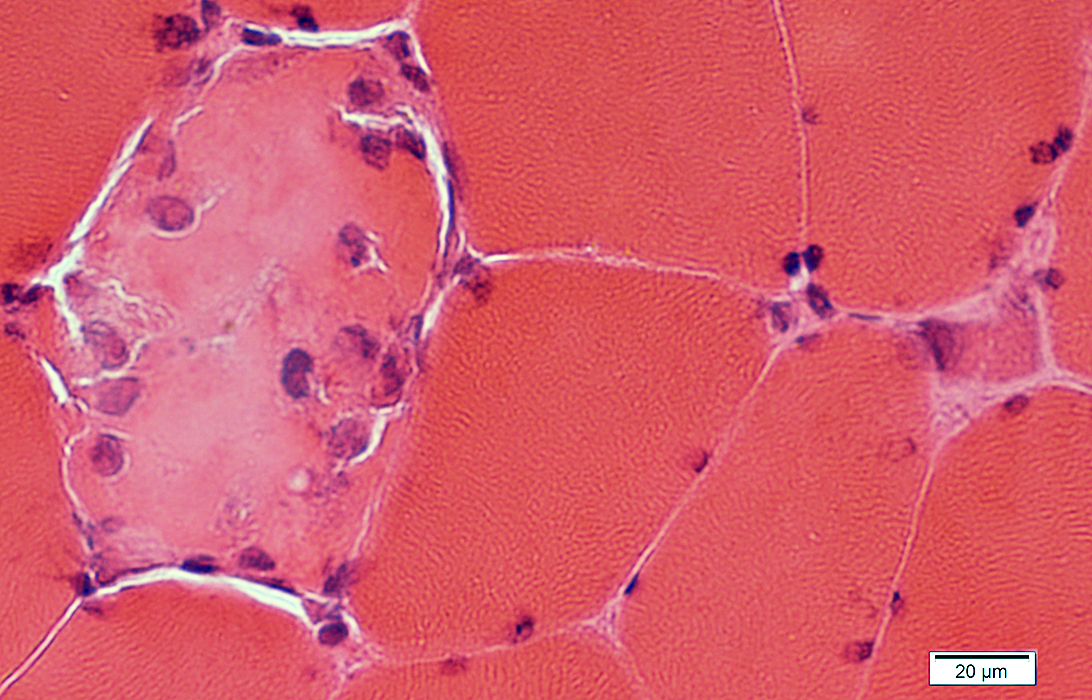
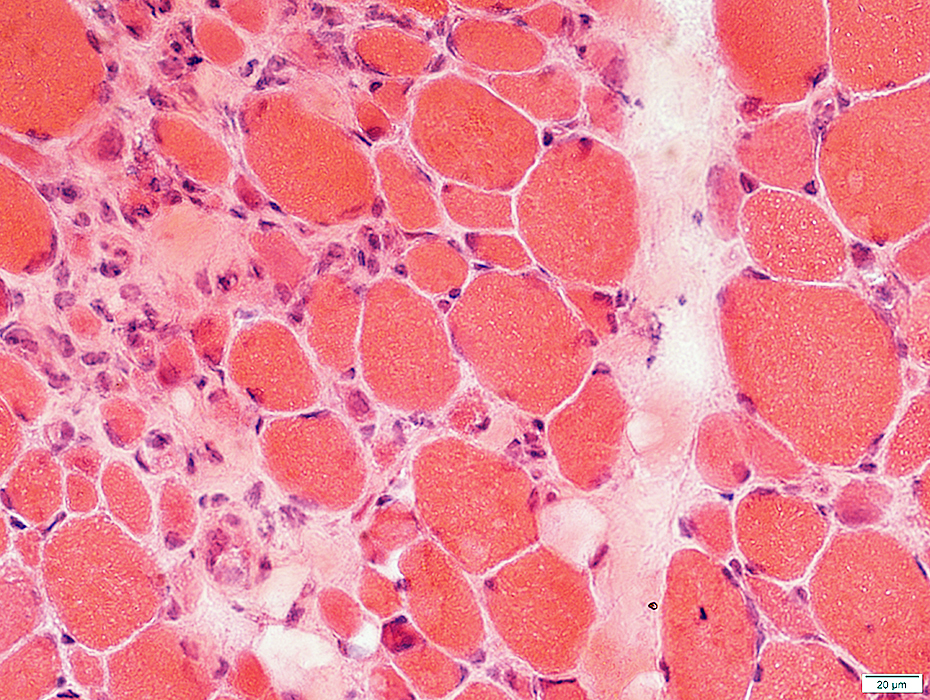
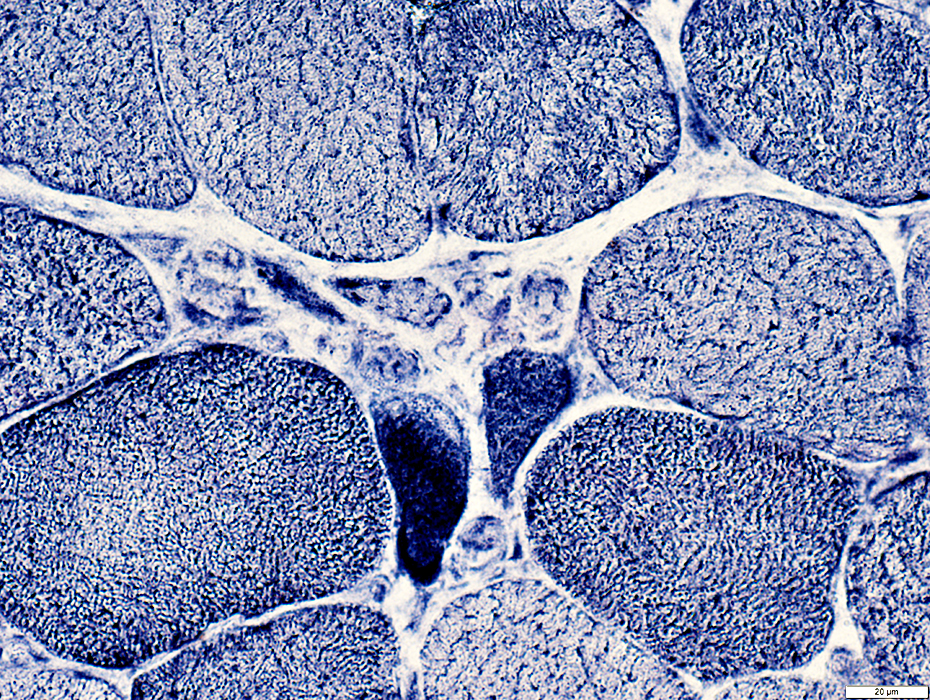
SRP: Early Pathology
Necrotic & Regenerating muscle fibers: Scattered
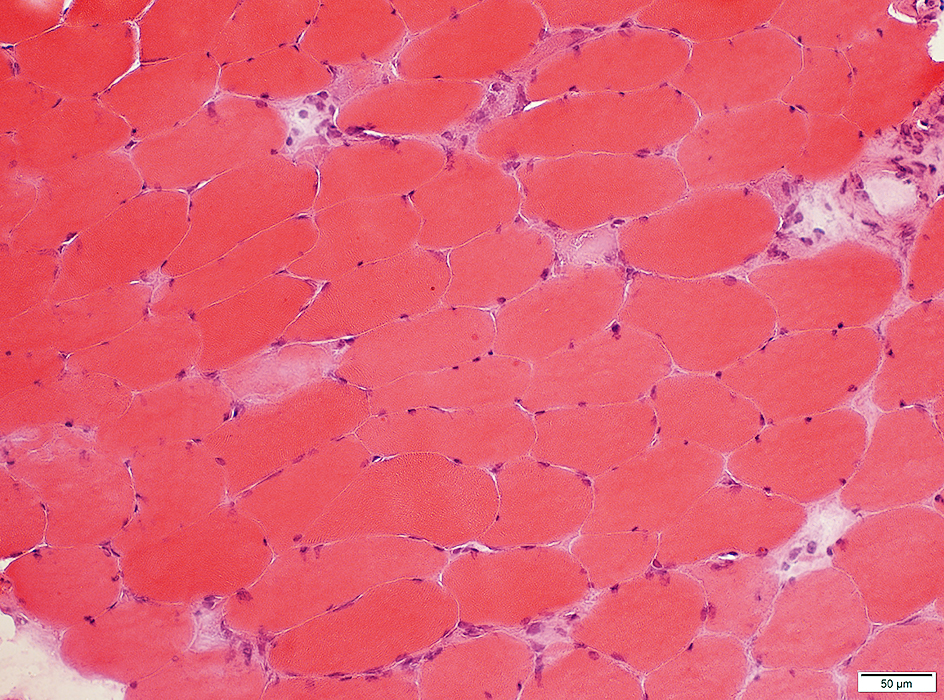 H&E stain |
|
Necrotic & Regenerating (Arrow) muscle fibers: Scattered
| ||
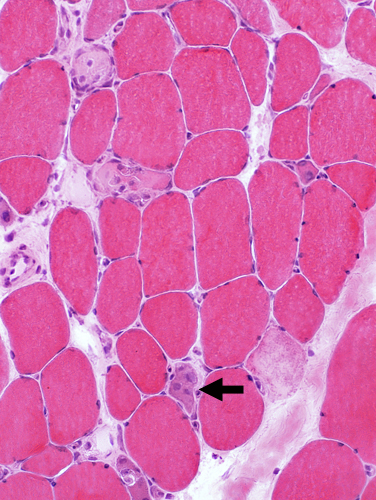 H&E stain |
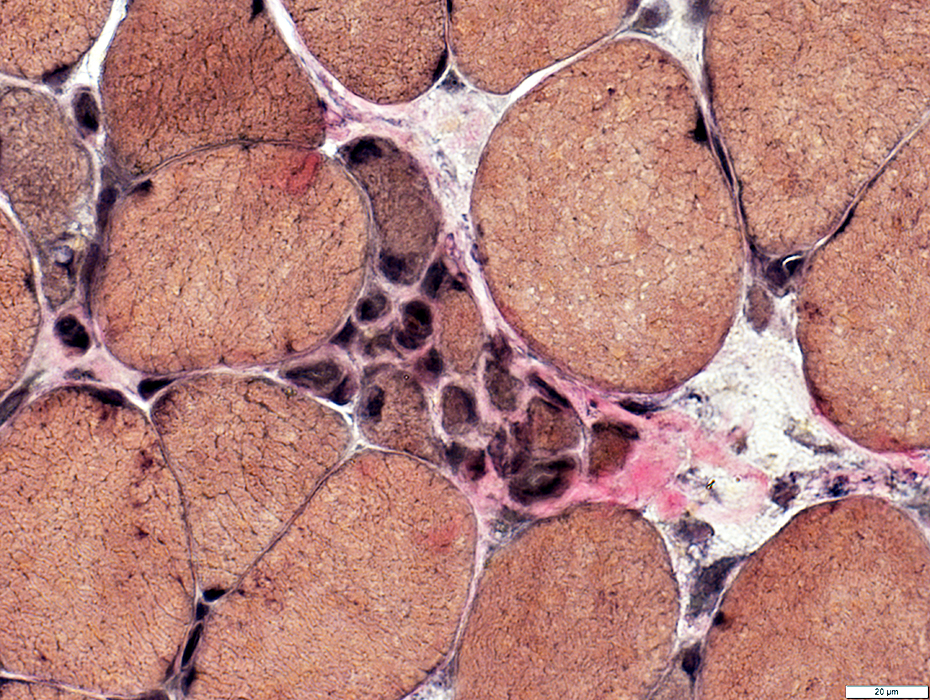
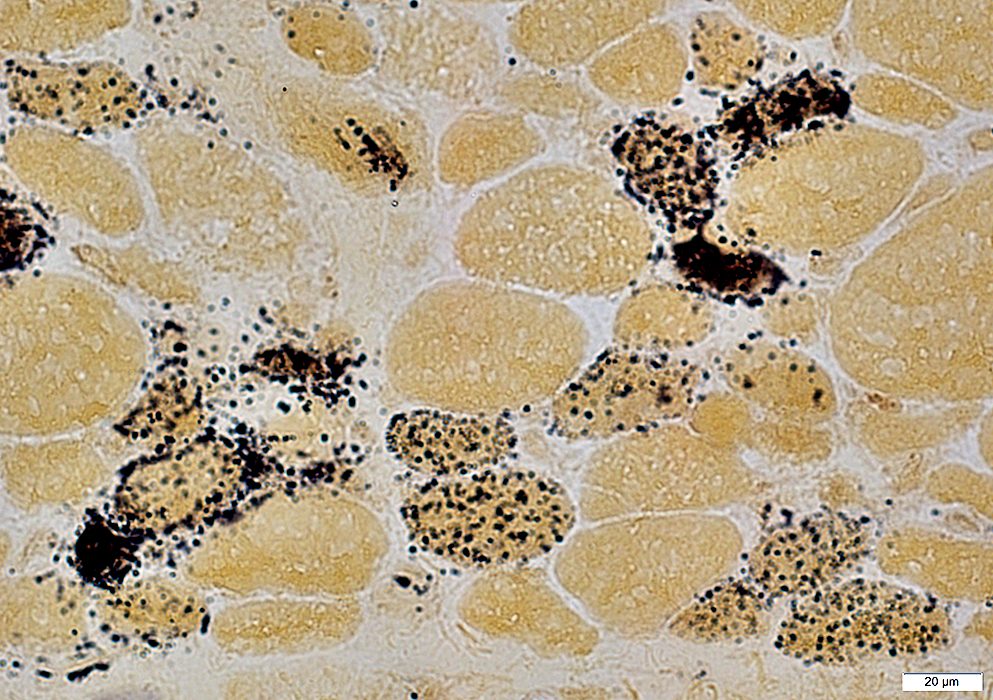
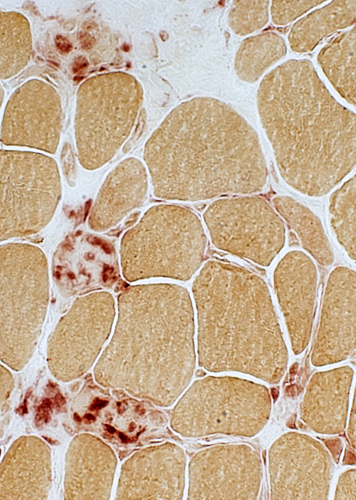 Acid phosphatase stain |
 Acid phosphatase stain |
 H&E stain |
 Congo red stain |
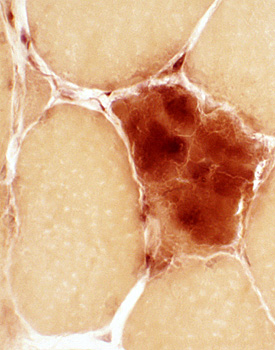
 Acid phosphatase stain |
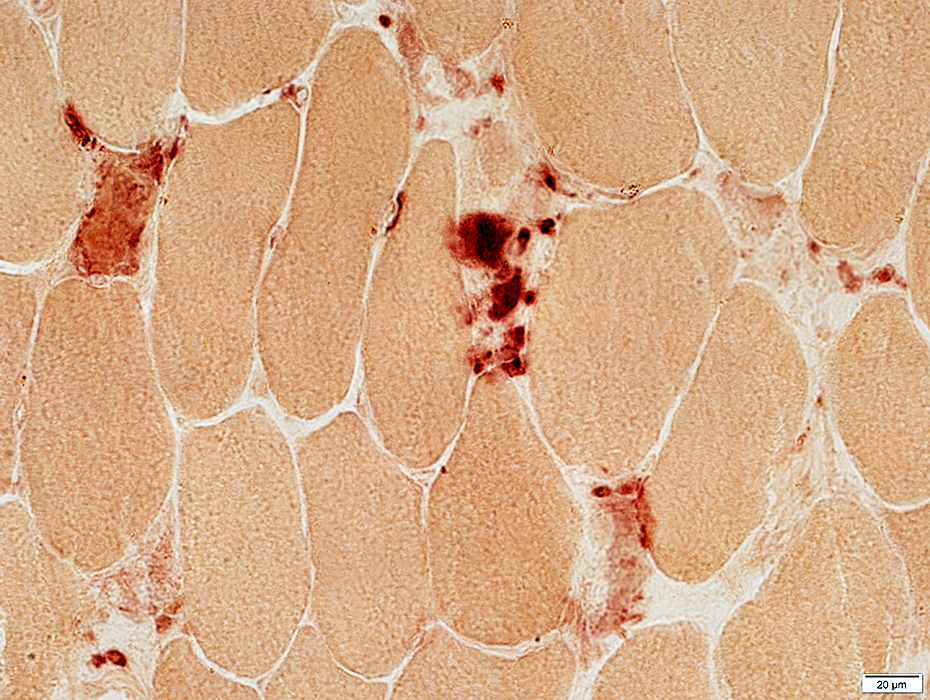
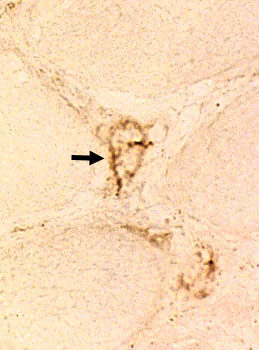
Phagocytic cells: Stain for acid phosphatase
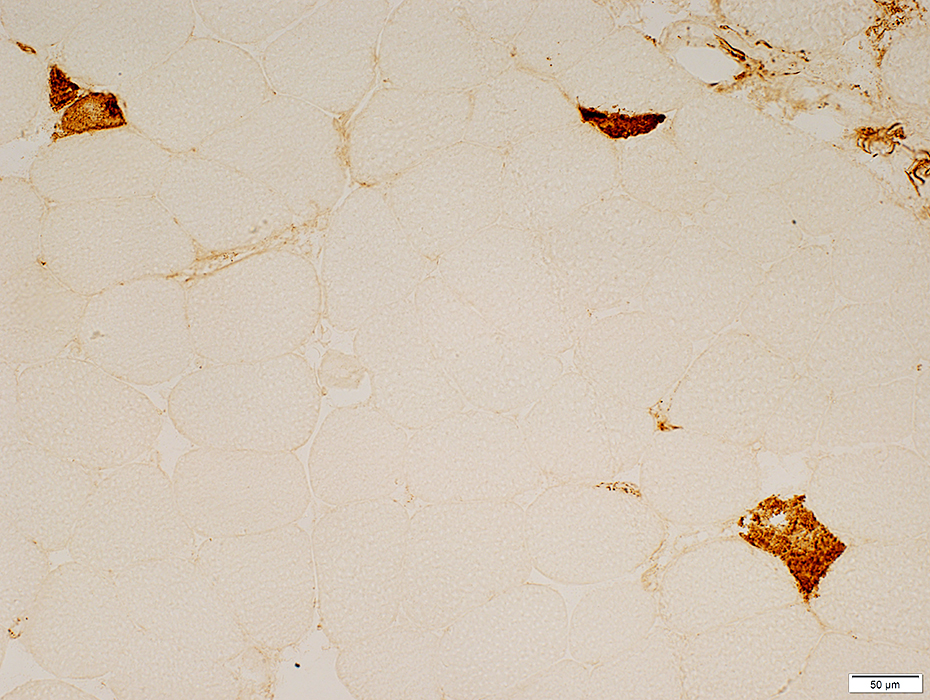
Cytoplasm: Stains for C5b-9 complement
 C5b-9 stain |
 NADH stain |
 NADH stain |
MHC Class I
Muscle fibers
Generally not expressed
Present in cytoplasm of regenerating muscle fibers
Cells: Present on histiocytic cells associated with necrotic muscle fibers
Vessels: Normally present on endomysial capillary & perimysial vessel endothelial cells
 MHC Class I stain |
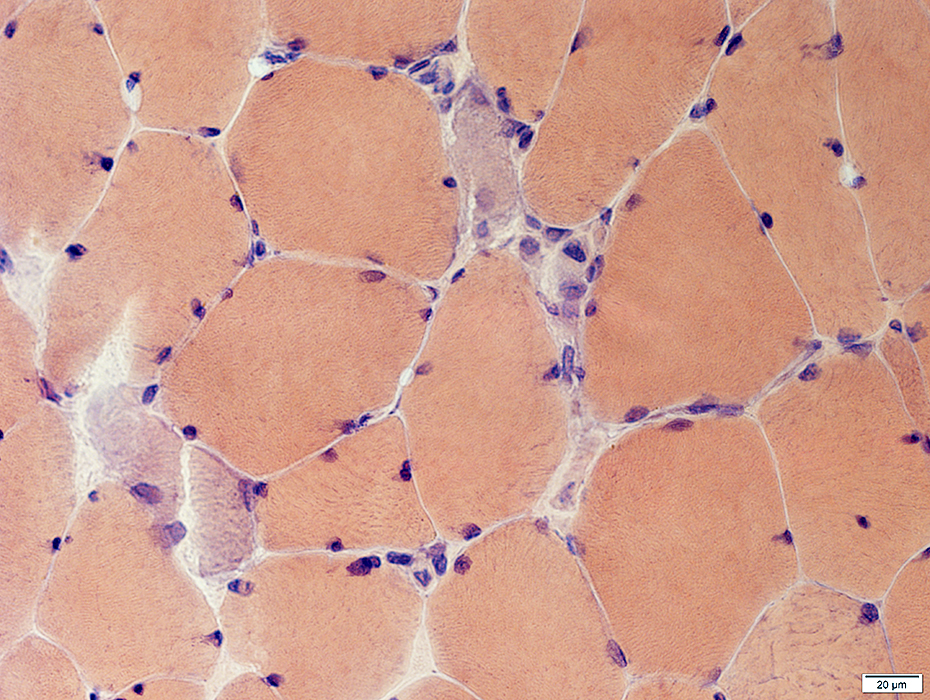
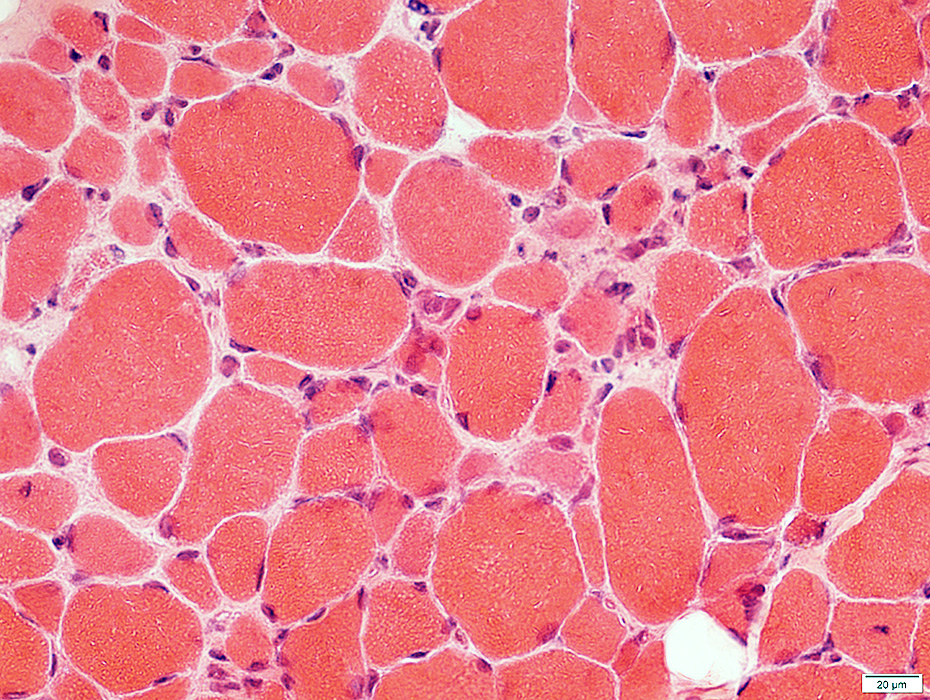
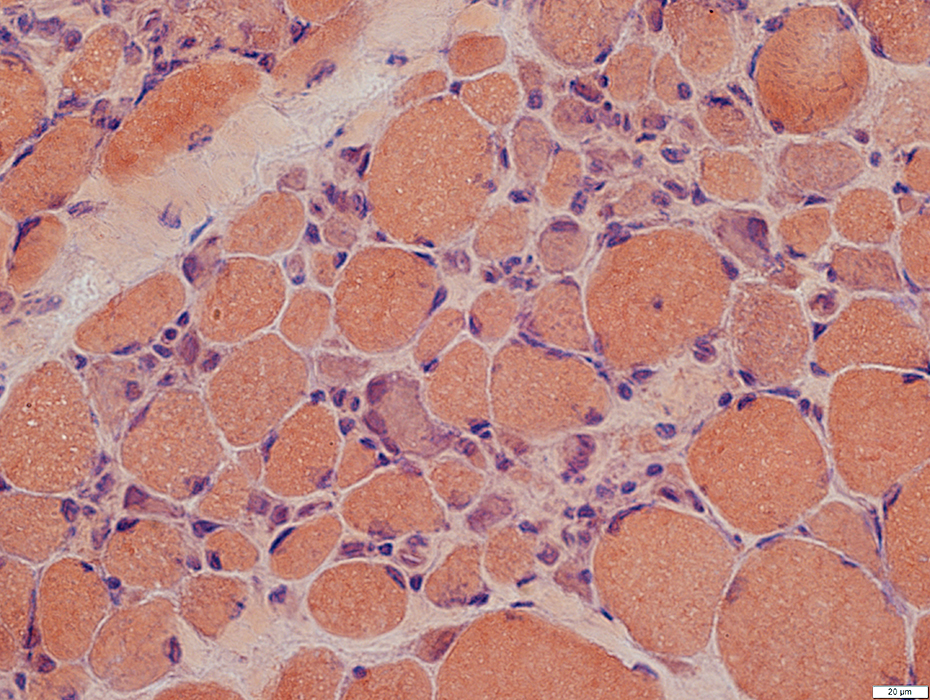
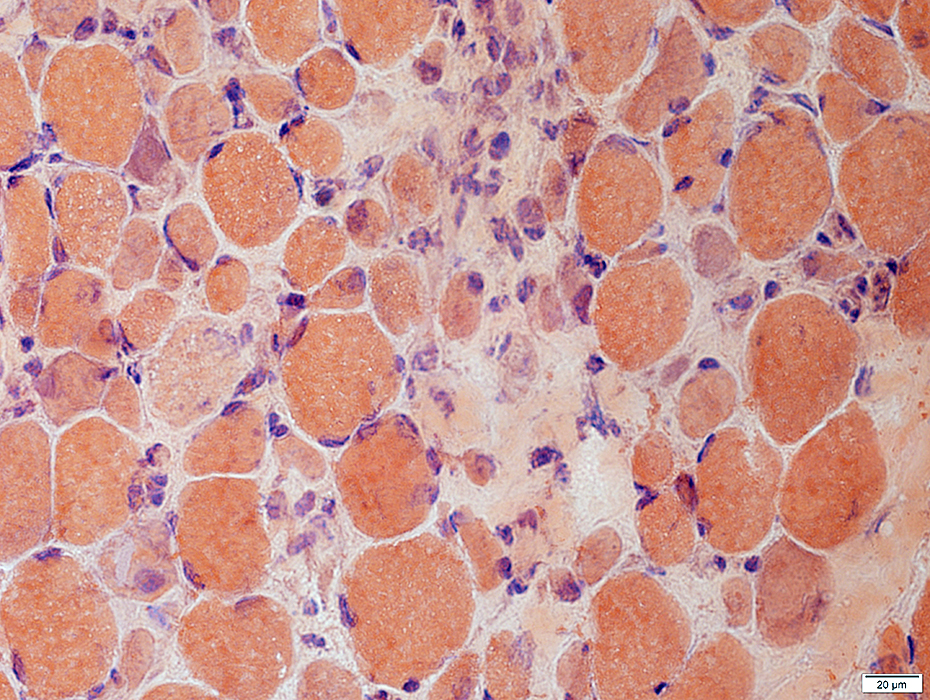
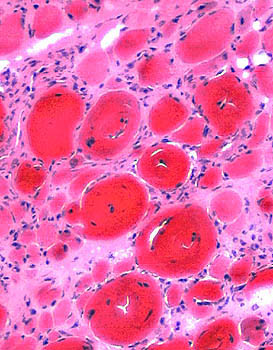
SRP: INTERMEDIATE PATHOLOGY
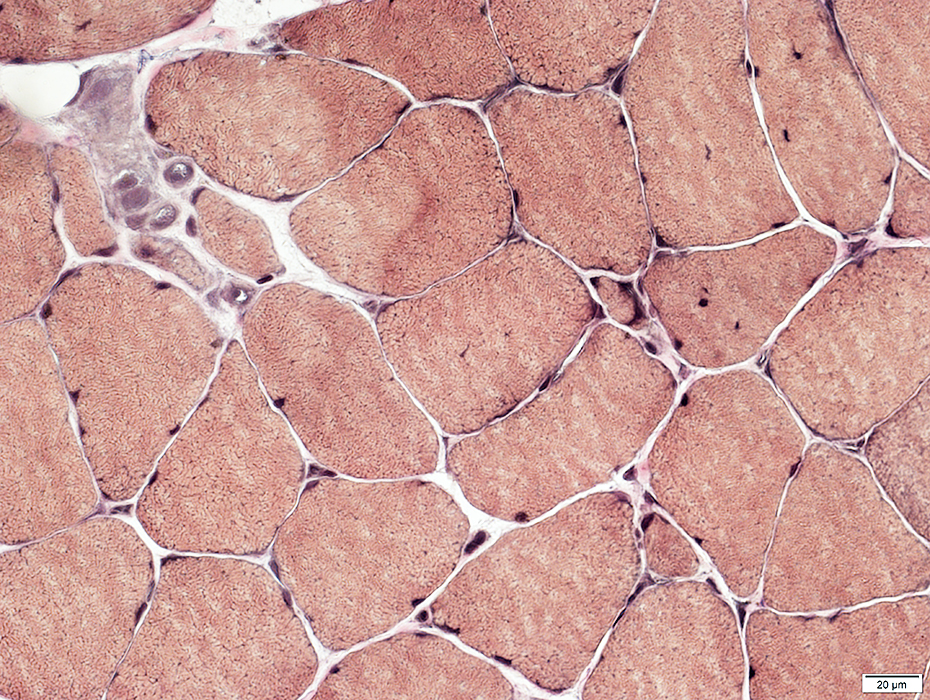
Muscle fiber sizes: Varied; Small to Upper limit of normal; Bimodal distribution
Small muscle fibers: Rounded; Large nuclei; Basophilic cytoplasm, Clustered
Endomysial connective tissue: Increased, Mild to Moderate
Perimysial connective tissue: Irregular or fragmented
Pathology distribution: Patchy; Some regions with more small muscle fibers & Increased endomysial connective tissue
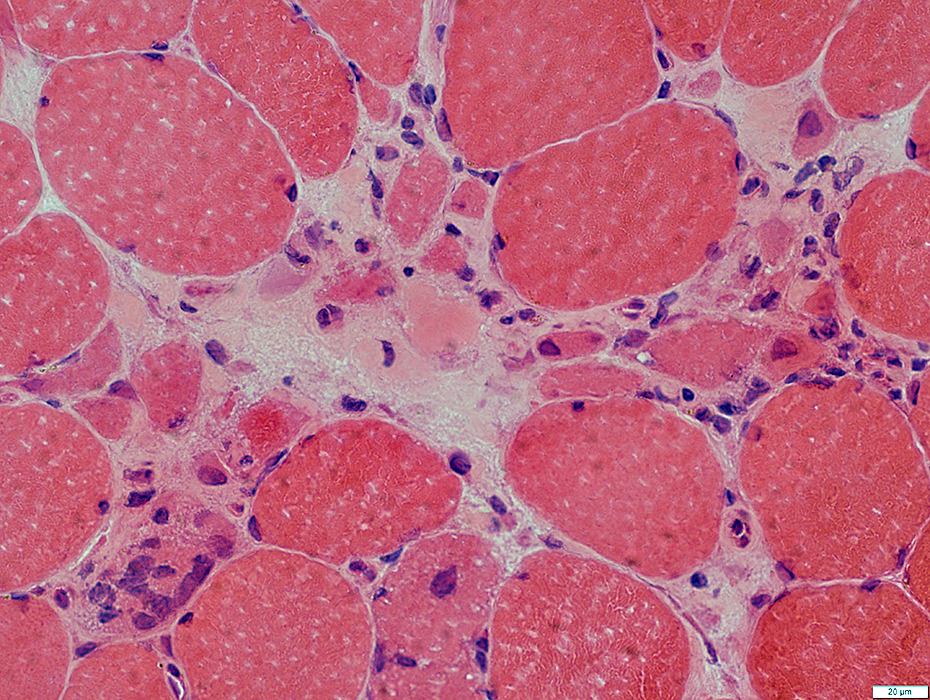
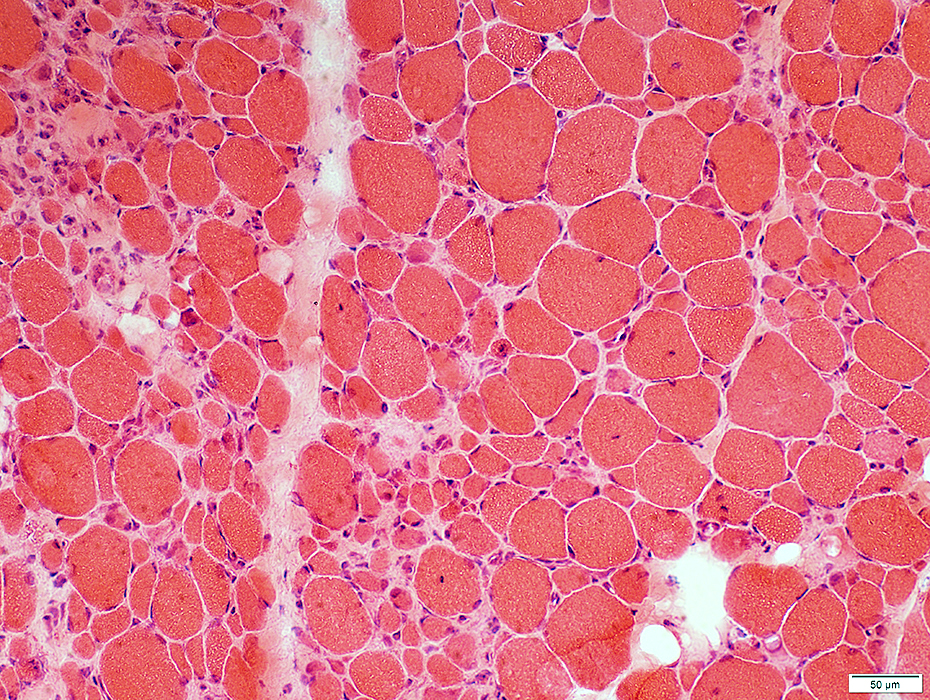 H&E stain |
Muscle damage
More severe, with increased endomysial connective tissue, in some regions
 H&E stain |
 H&E stain |
|
Muscle fiber sizes: Bimodal Small muscle fibers: Rounded; Large nuclei Endomysial connective tissue: Mildly increased |
 H&E stain |
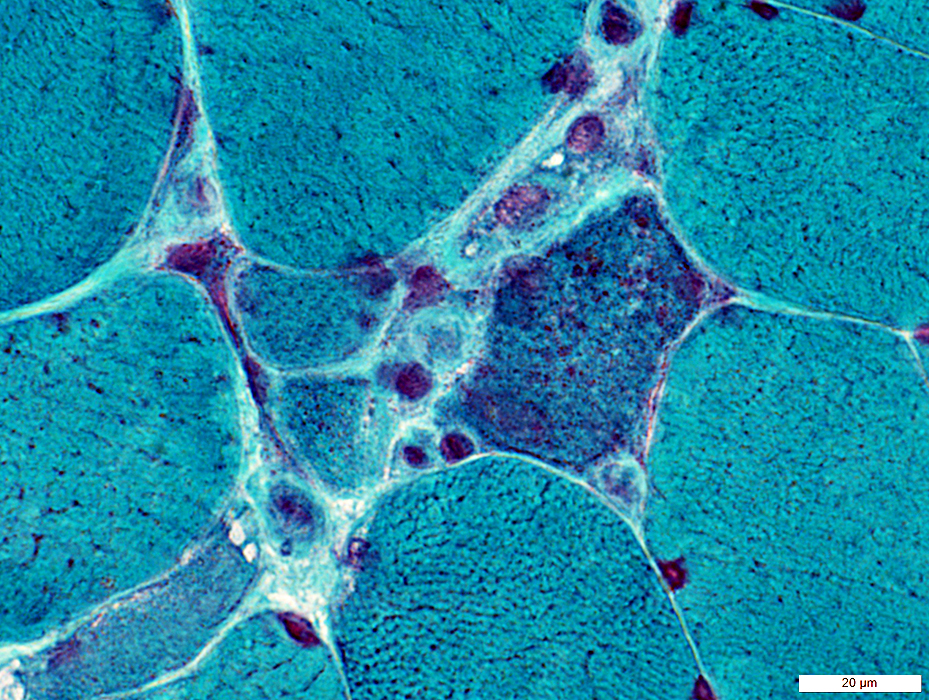
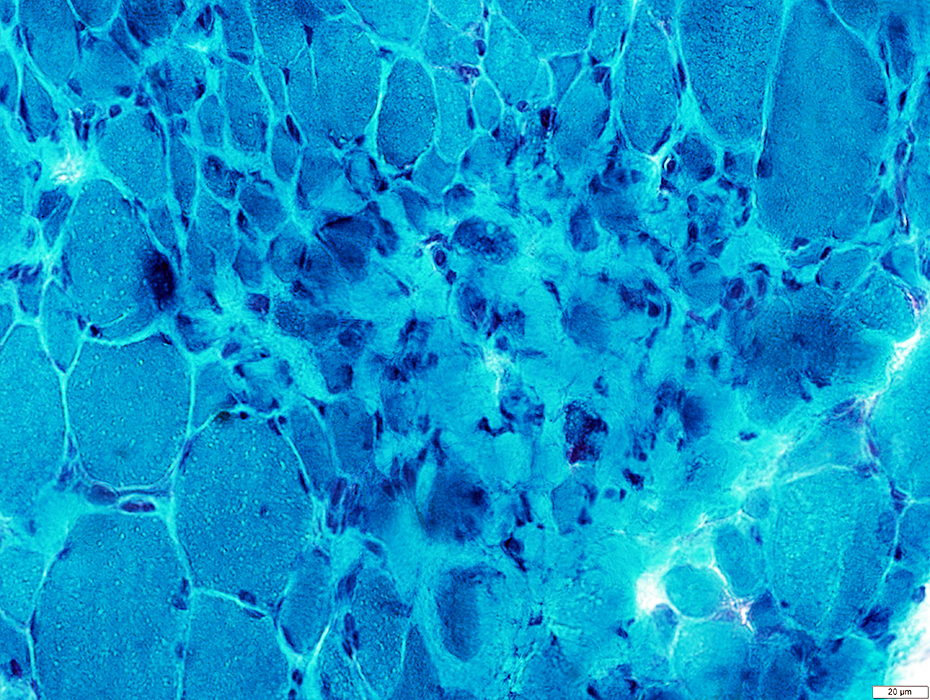
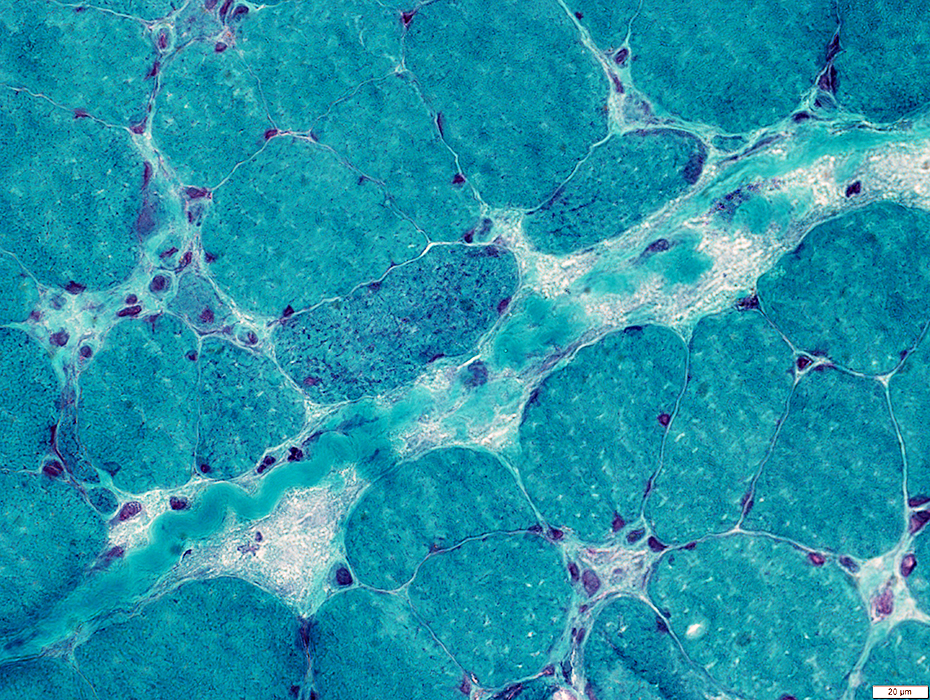
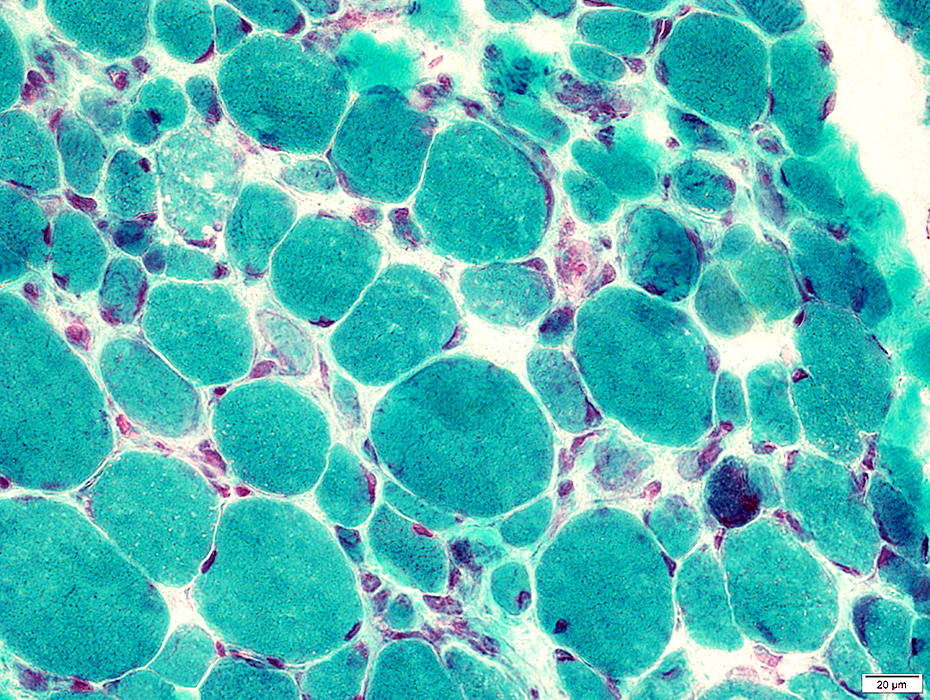 Gomori trichrome stain |
 Gomori trichrome stain |
 Congo red stain |
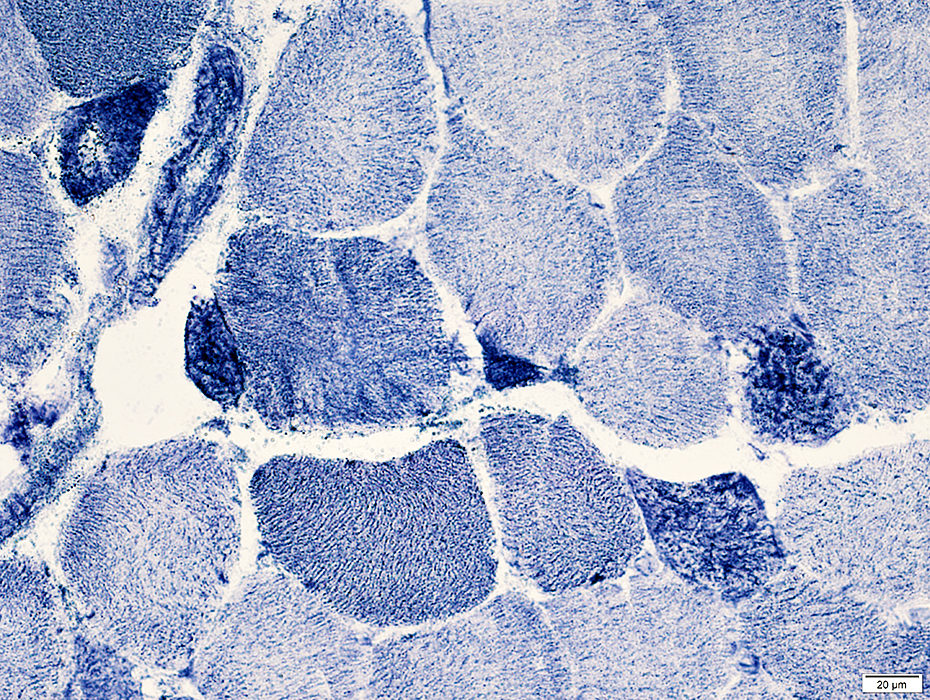
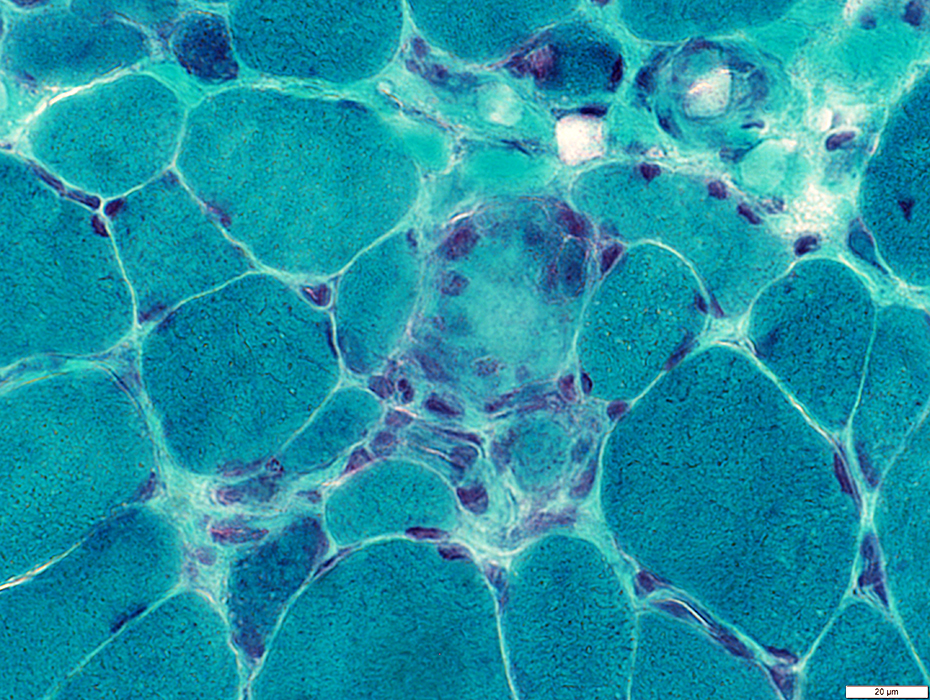
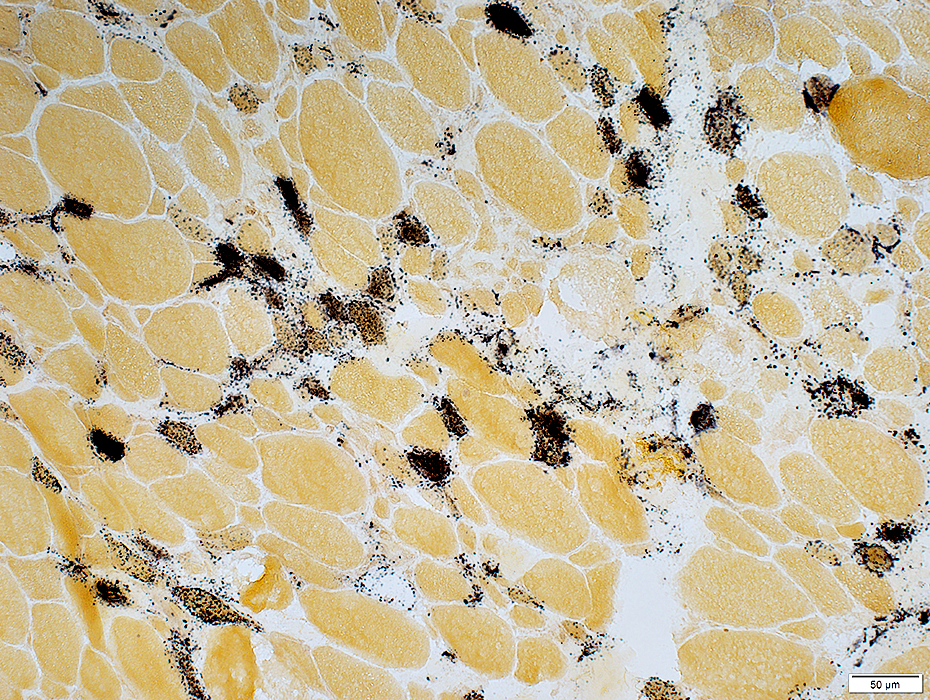
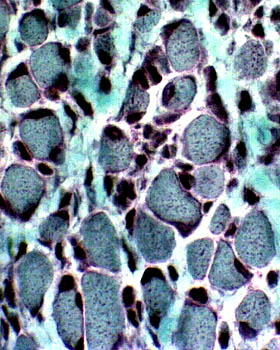
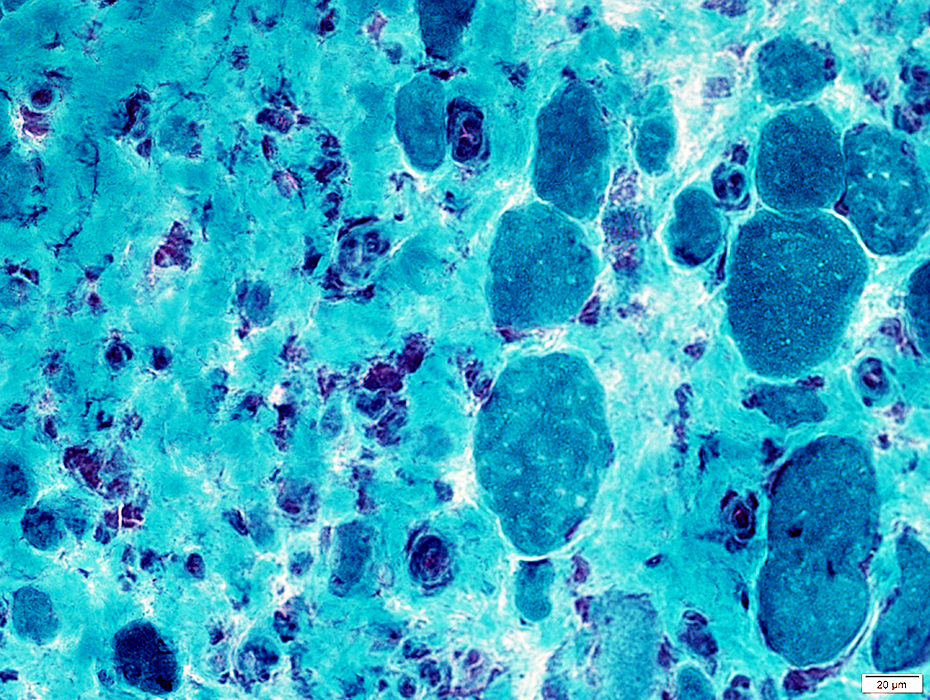
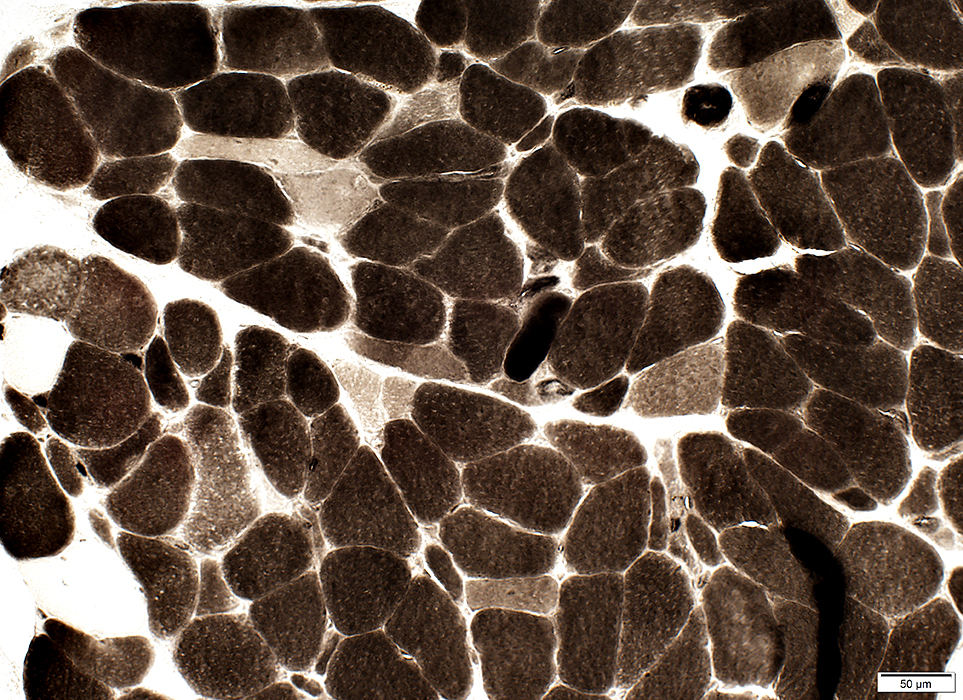
Muscle fiber internal architecture
Some small muscle fibers stain dark
One necrotic muscle fiber has pale cytoplasm (Arrow)
Large fibers have coarse internal architecture
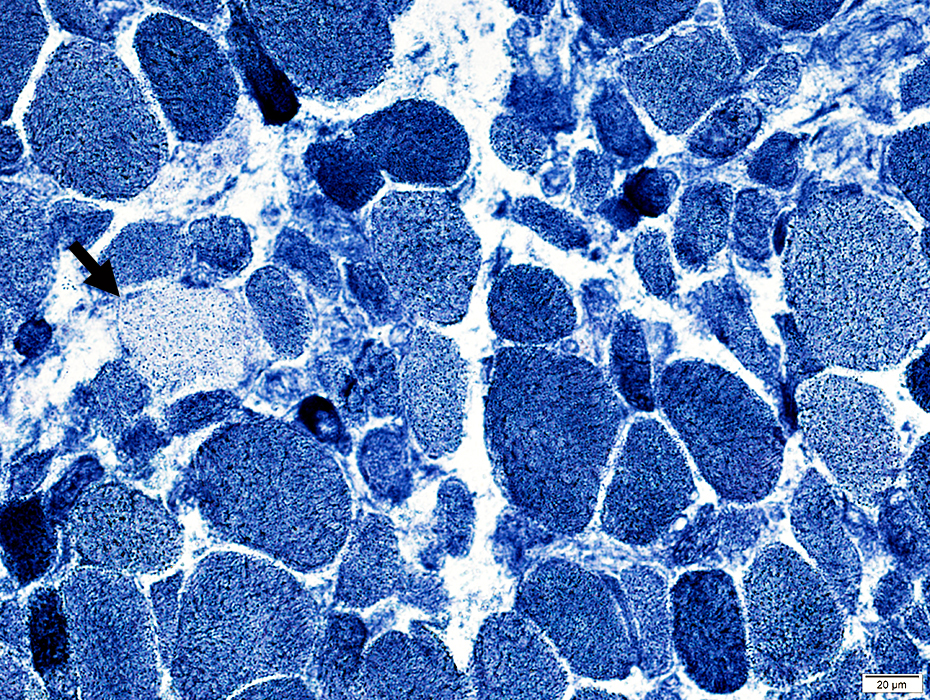 NADH stain |
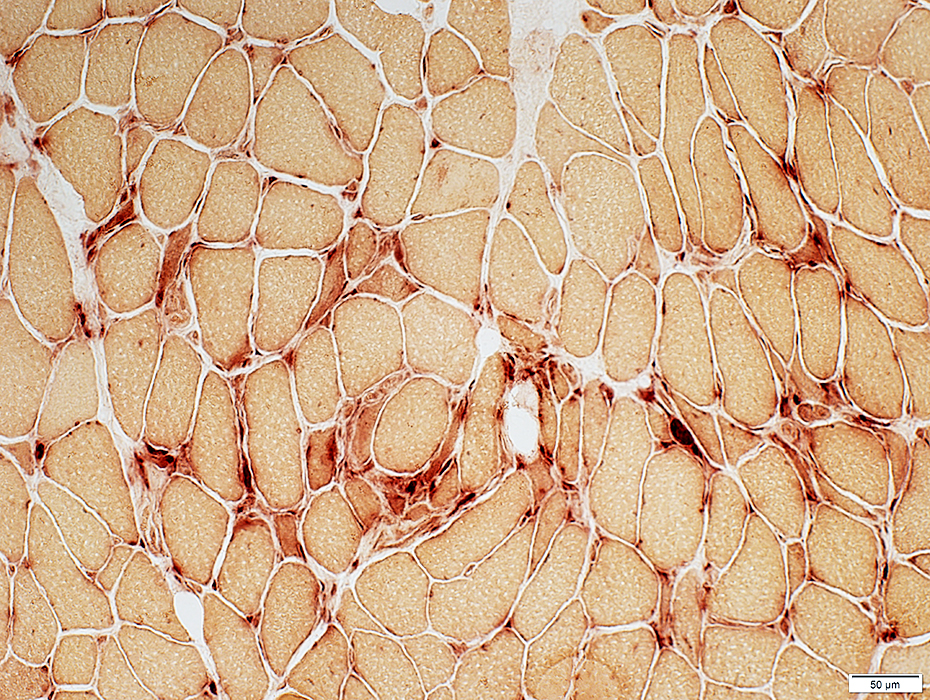
 VvG stain |
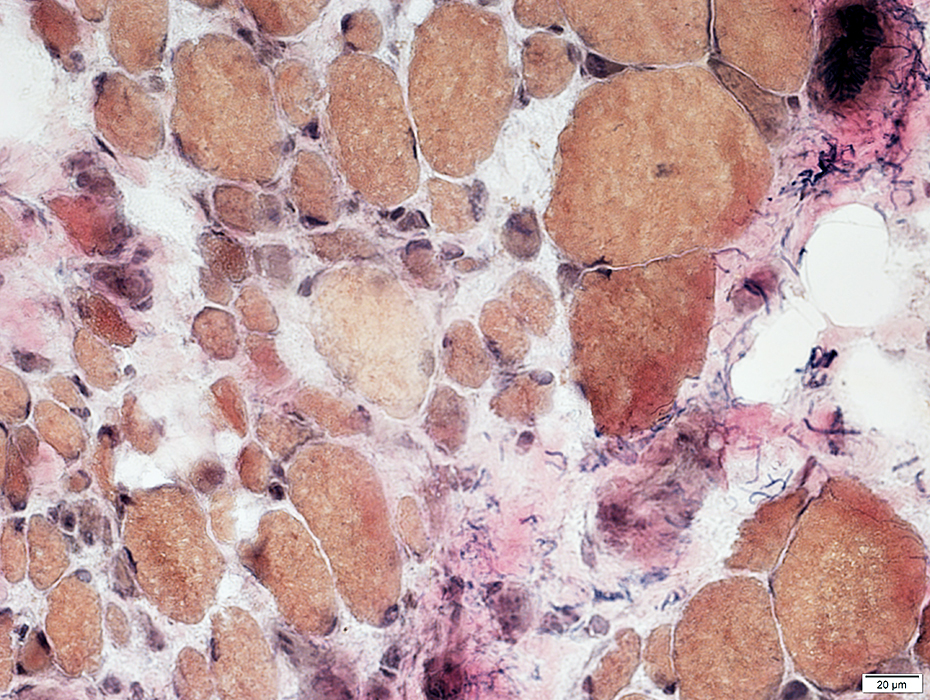
Endomysial connective tissue: Increased
Muscle fiber necrosis: Few fibers with pale-stained cytoplasm
 Congo red stain |
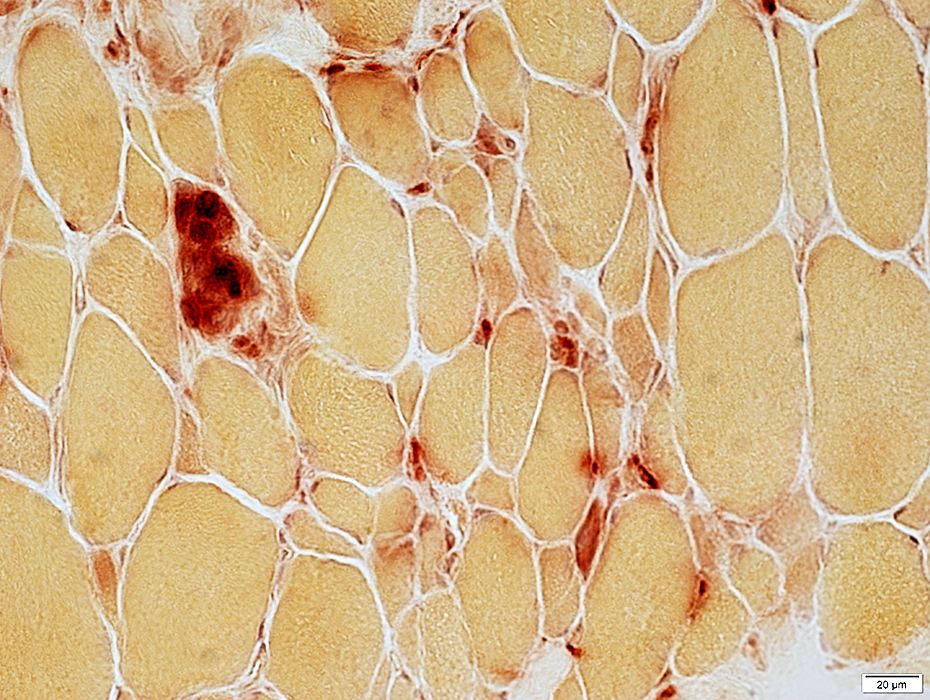
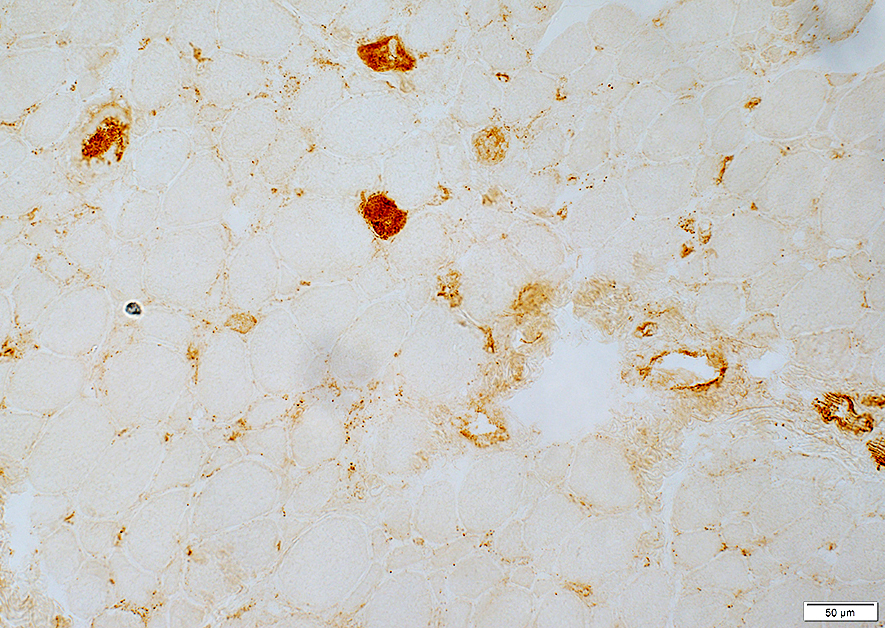
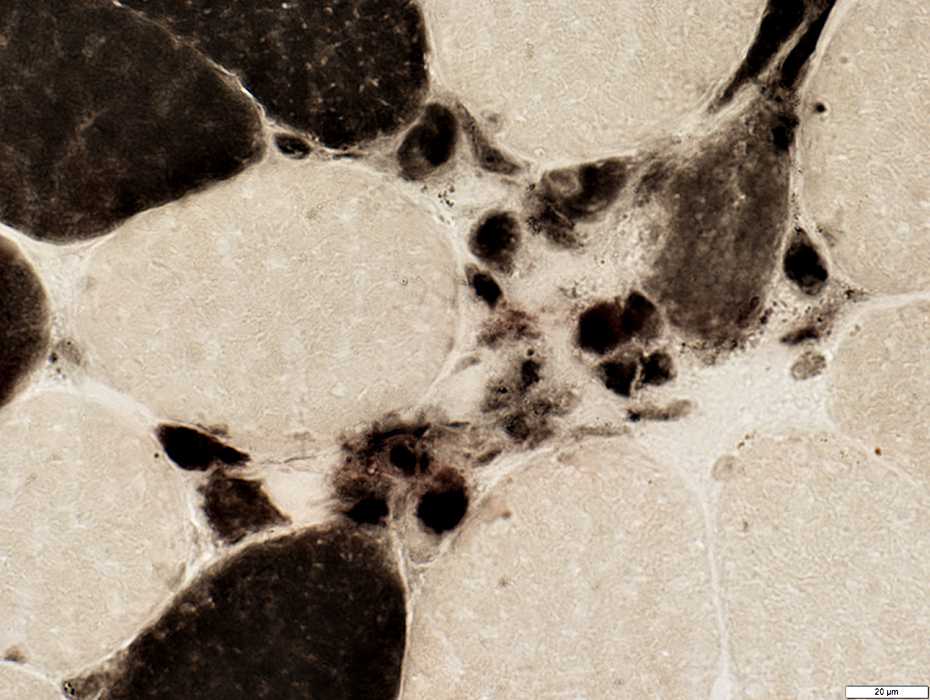
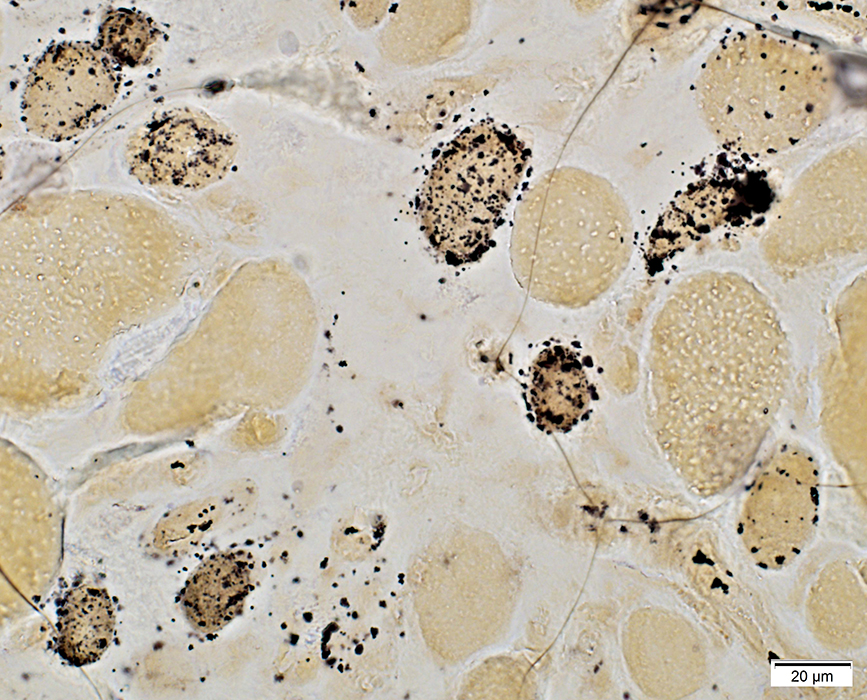
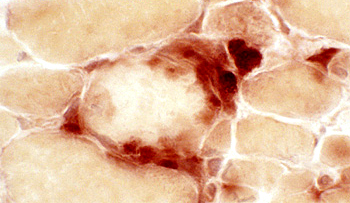 Acid phosphatase stain Necrotic muscle fibers Scattered Pale cytoplasm Associated histiocytic cells |
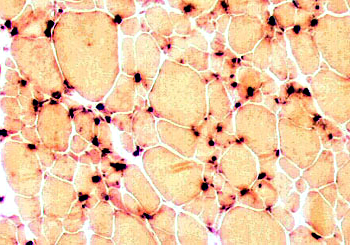 Acid phosphatase stain Acid phosphatase positive cells Scattered in endomysium |
 Acid phosphatase stain |
Necrotic muscle fibers
Scattered in muscle
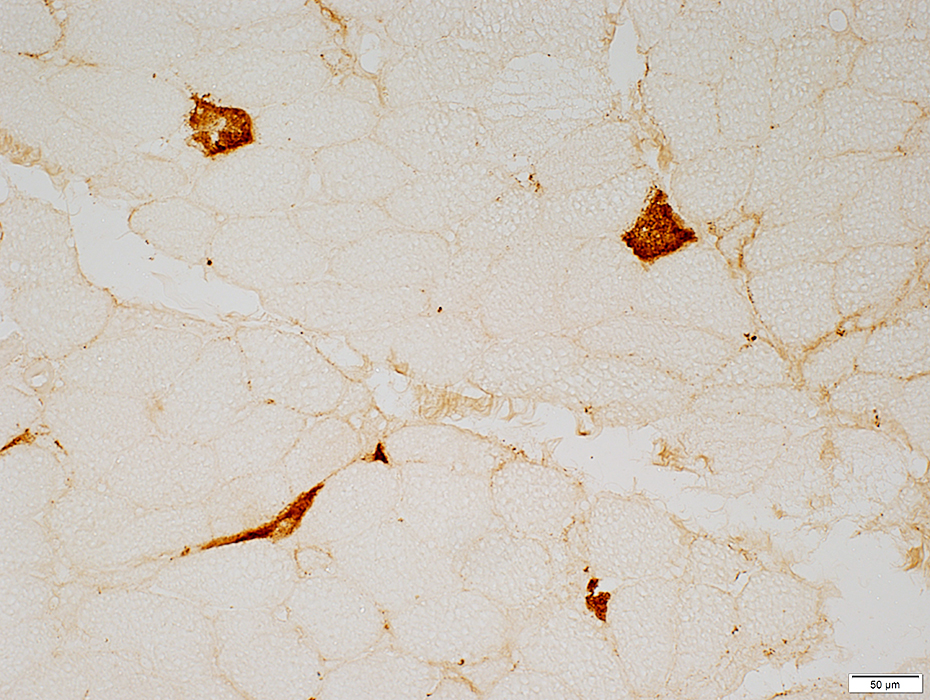
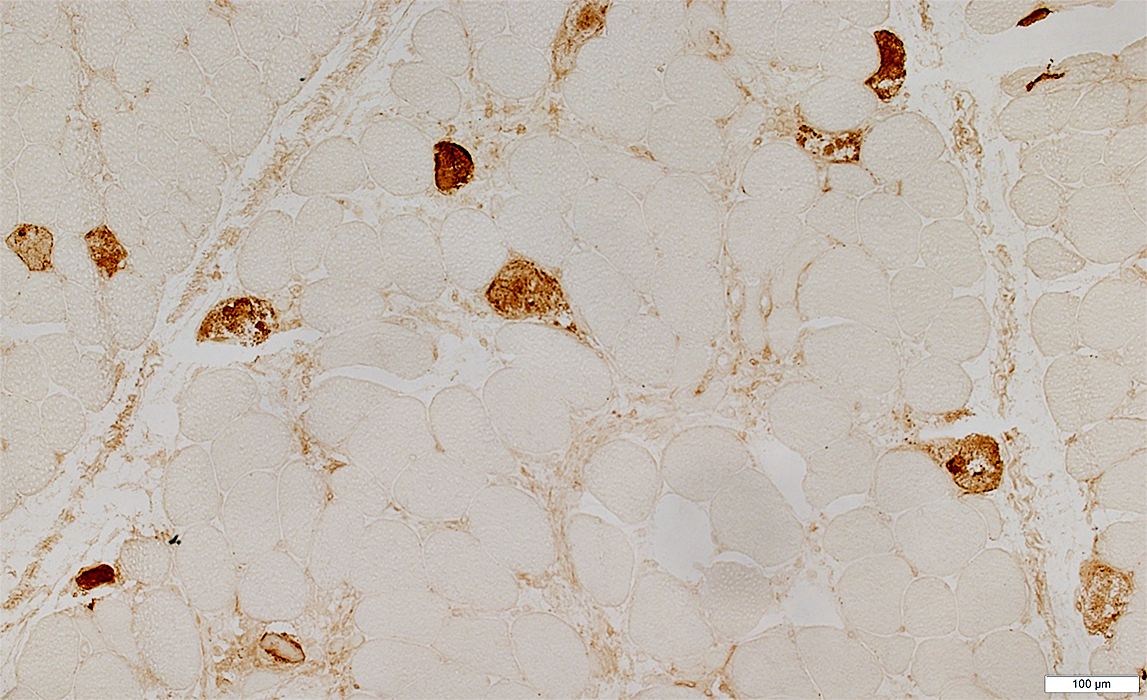 C5b-9 stain |
Necrotic muscle fibers
Distribution: Scattered
Cytoplasm: Diffuse C5b-9 stain
Endomysial capillaries: Some patients
 C5b-9 stain |
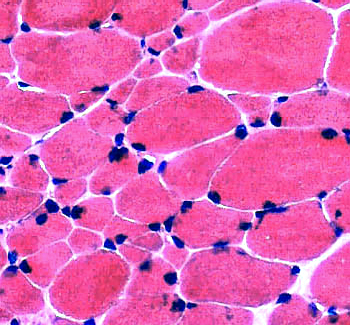
SRP myopathy: Immature muscle fibers
Many muscle fibers persist in immature states
 Alkaline phosphatase stain |
Properties
Many small immature muscle fibers stain for alkaline phosphatase
Many small & large muscle fibers are type 2C (Below)
Distribution in muscle: Immature, small fibers are often clustered
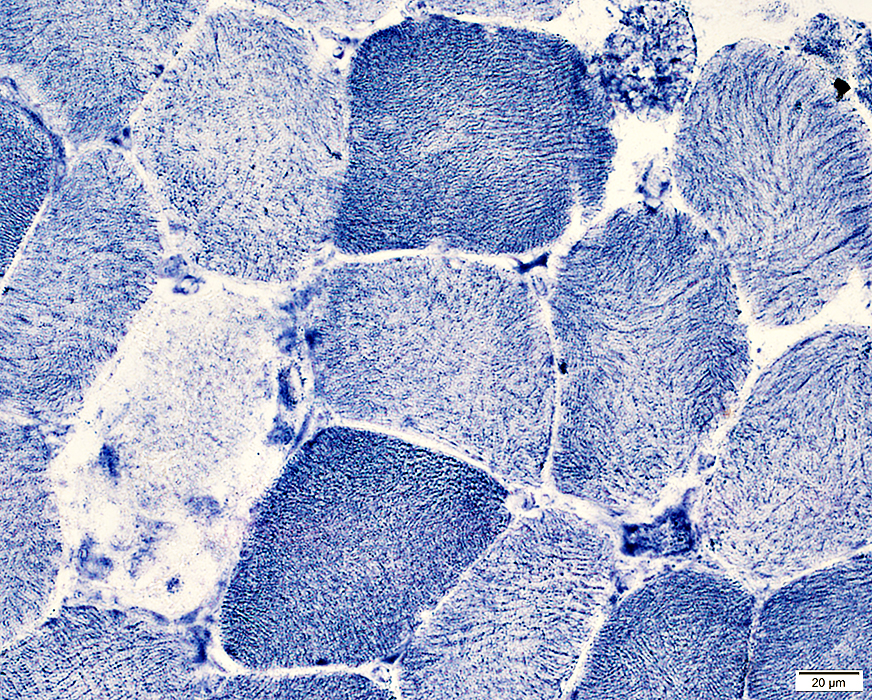
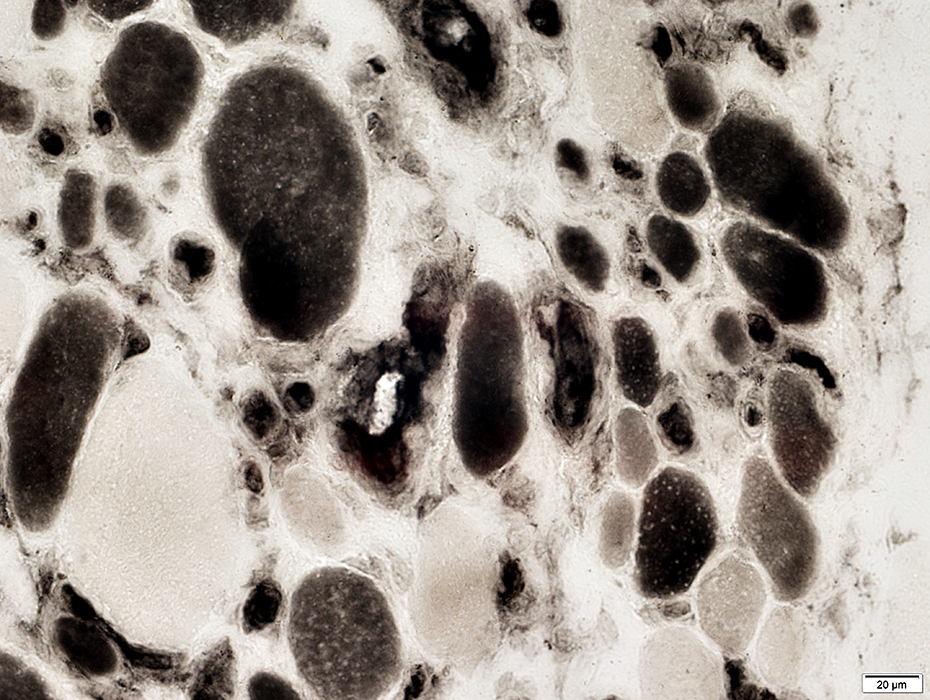
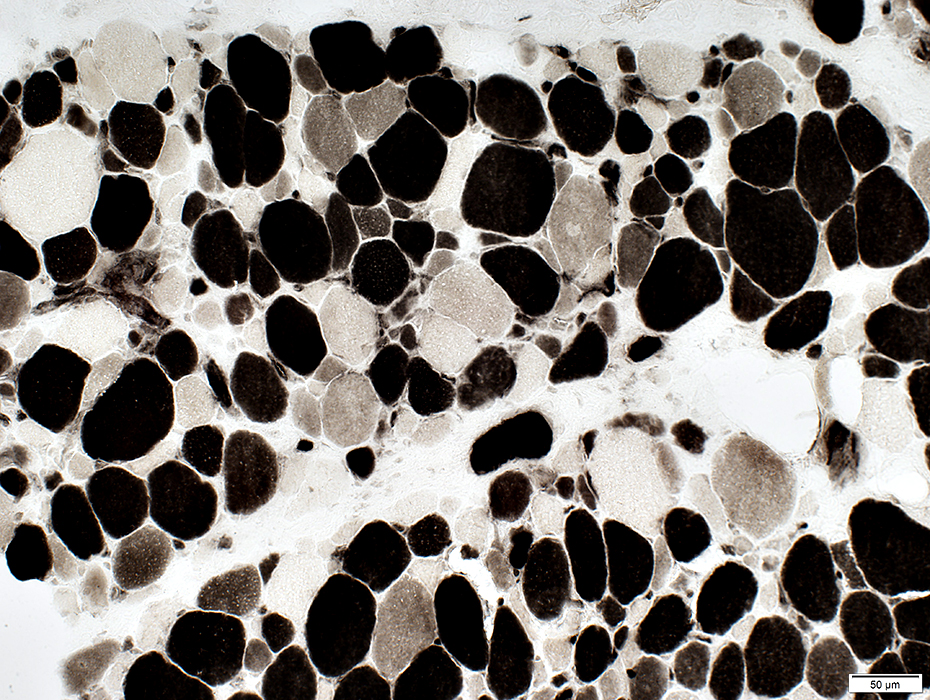 ATPtase pH 4.3 stain |
Immature Muscle Fibers: Clustered
 ATPtase pH 4.3 stain |
 H&E stain |
 Gomori trichrome stain |
 VvG stain |
 NADH stain |
 Alkaline phosphatase stain |
 Gomori trichrome stain |
 VvG stain |
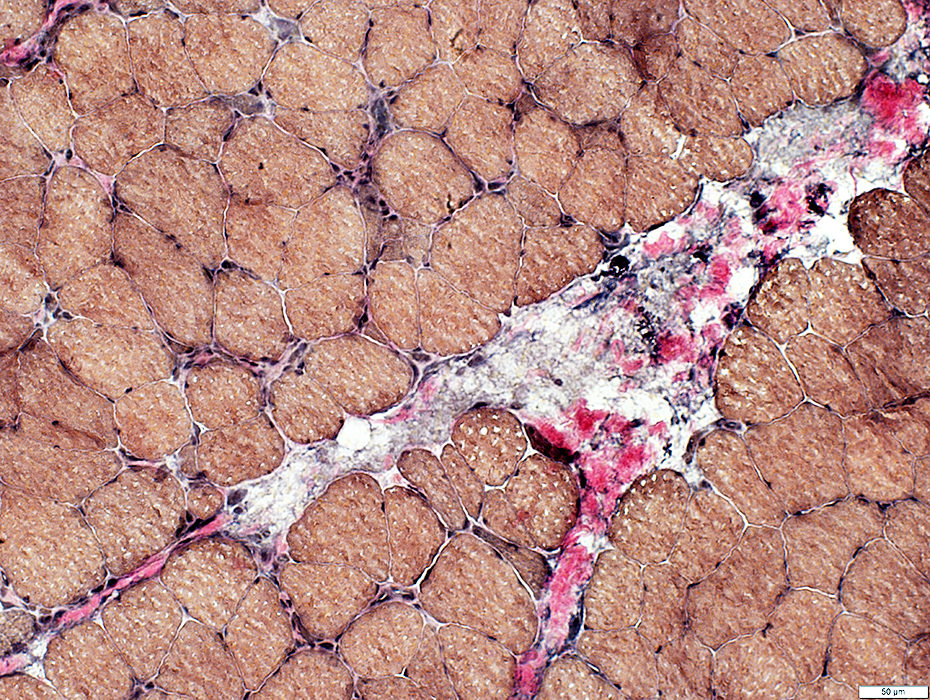
SRP Myopathy, Moderate
Perimysial Pathology
 Gomori trichrome stain |
Fragmented
No cells
 VvG stain |
 VvG stain |
SRP Myopathy, Moderate
Myofiber Basal Lamina Pathology
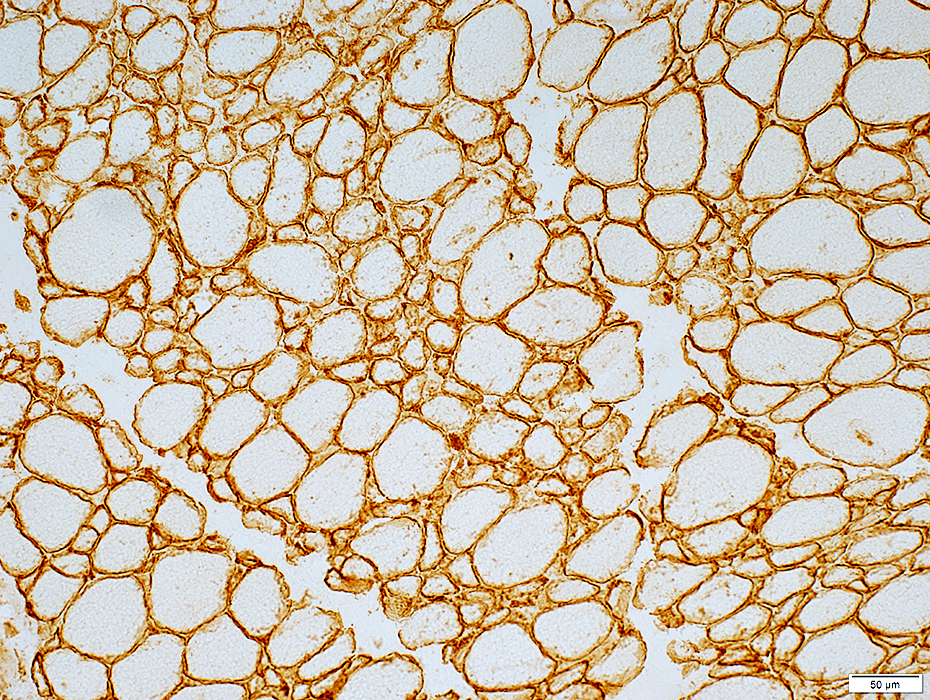 Laminin-α2 stain |
Control Muscle fiber basal lamina
 Laminin-α2 stain |
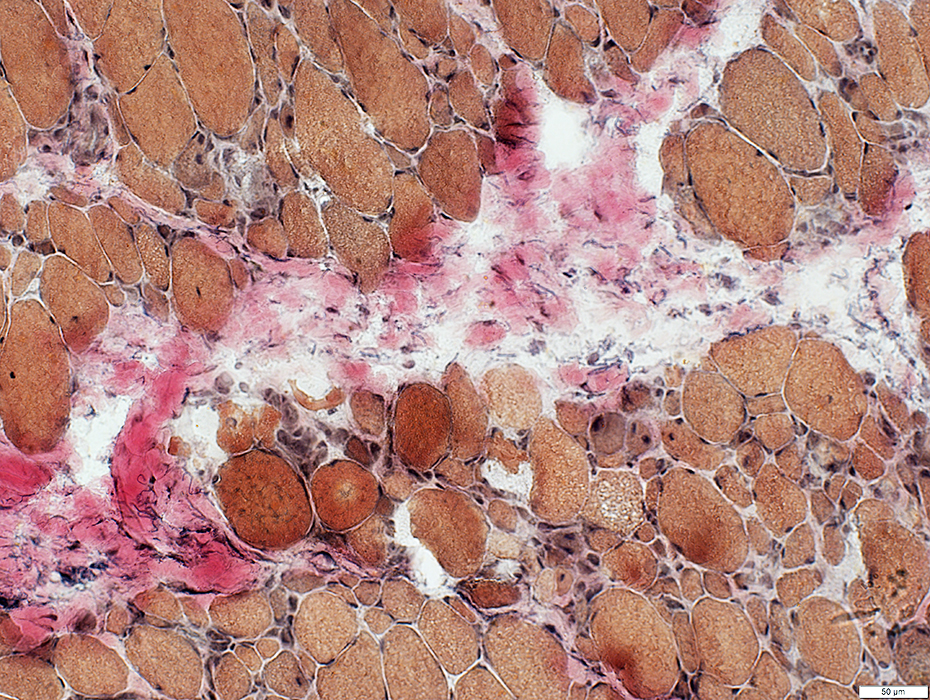
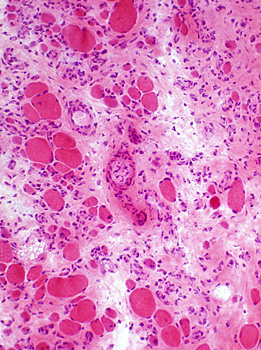
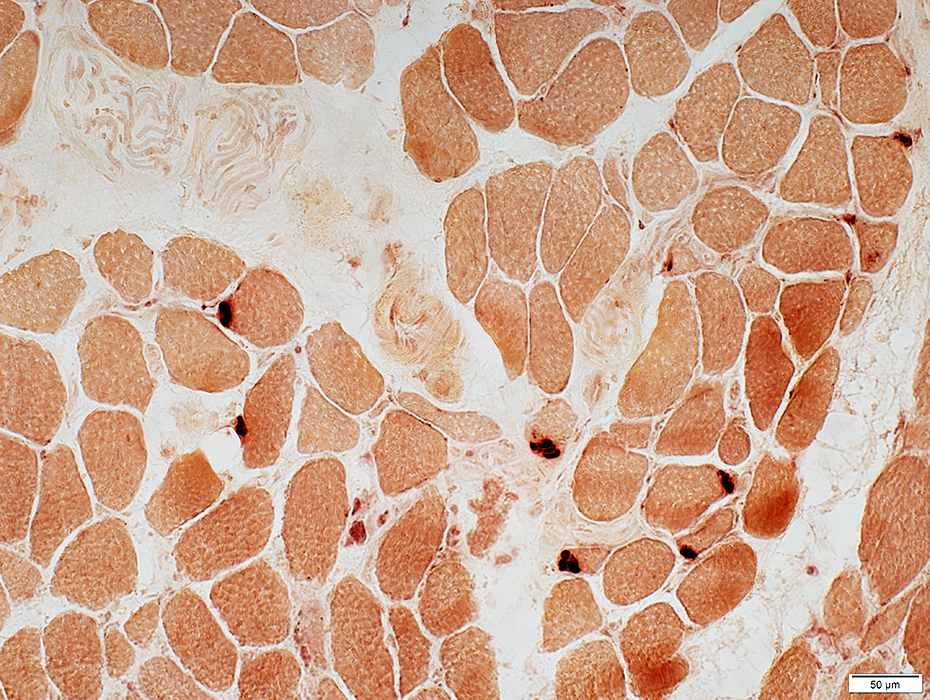
SRP: LATE, SEVERE PATHOLOGY, Months
Muscle fiber sizes: Varied; Small to Mildly large
Small muscle fibers: Rounded; Large nuclei; Basophilic cytoplasm
Endomysial connective tissue: Increased, Moderate to Marked
Pathology distribution: Patchy; Some regions with more endomysial connective tissue & only small rounded muscle fibers
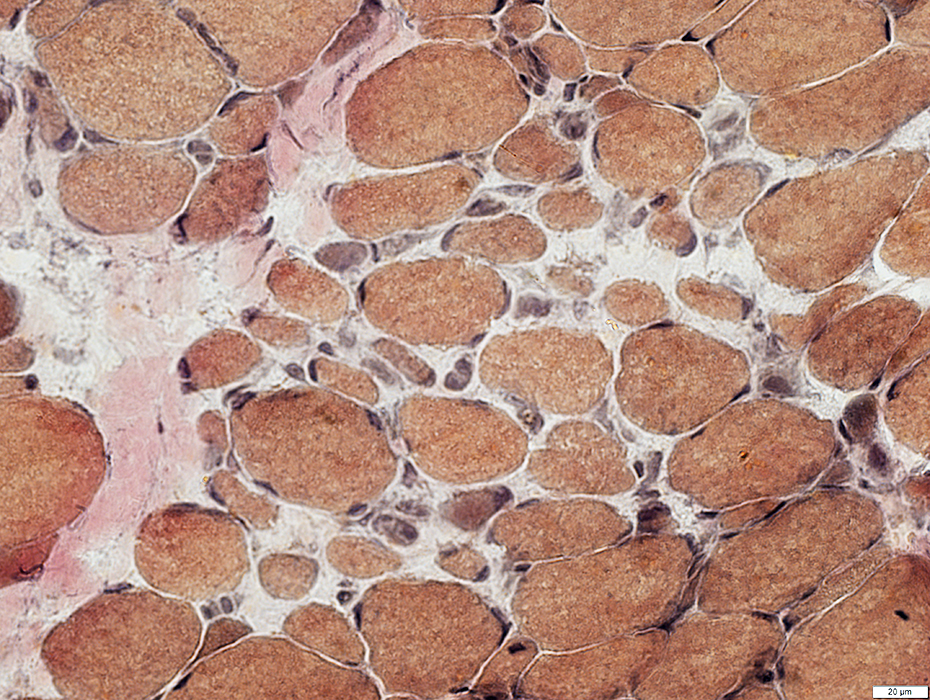
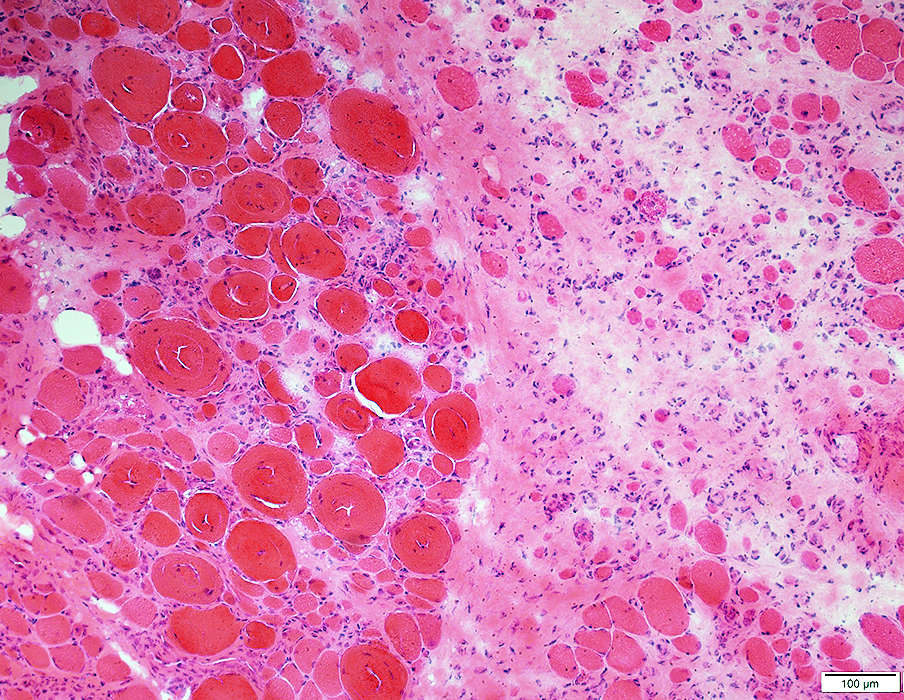 H&E stain |
 H&E stain Increased endomysial connective tissue Hypertrophic and small muscle fibers |
 Gomori trichrome stain Many small rounded muscle fibers Increased endomysial connective tissue |
 H&E stain Endomysial connective tissue: Marked increase Disease course of only 6 months |
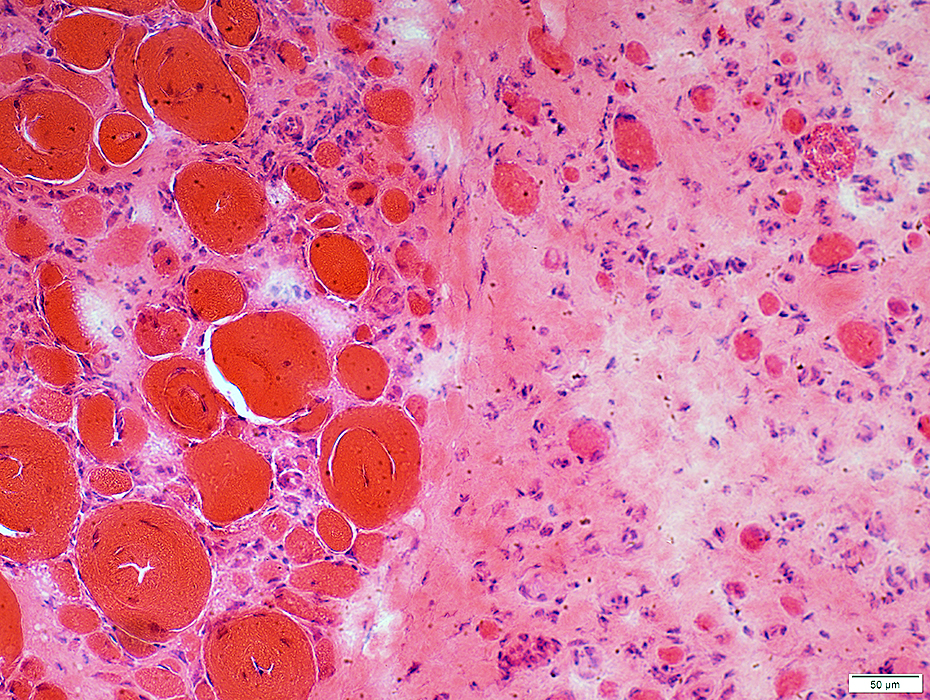 H& E stain |
Marked increase
More in some fascicles than others
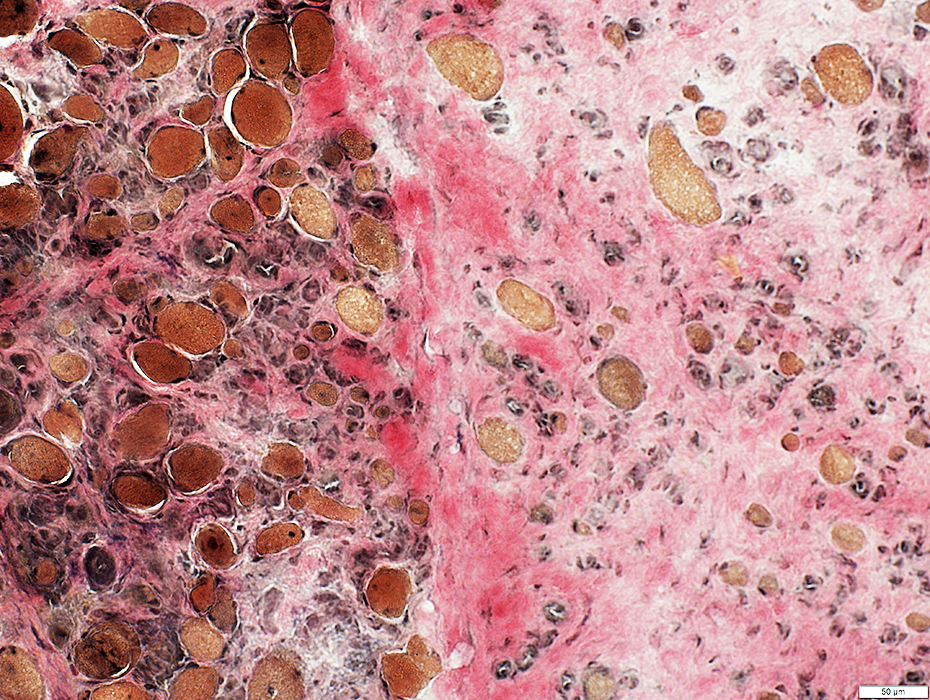 VvG stain |
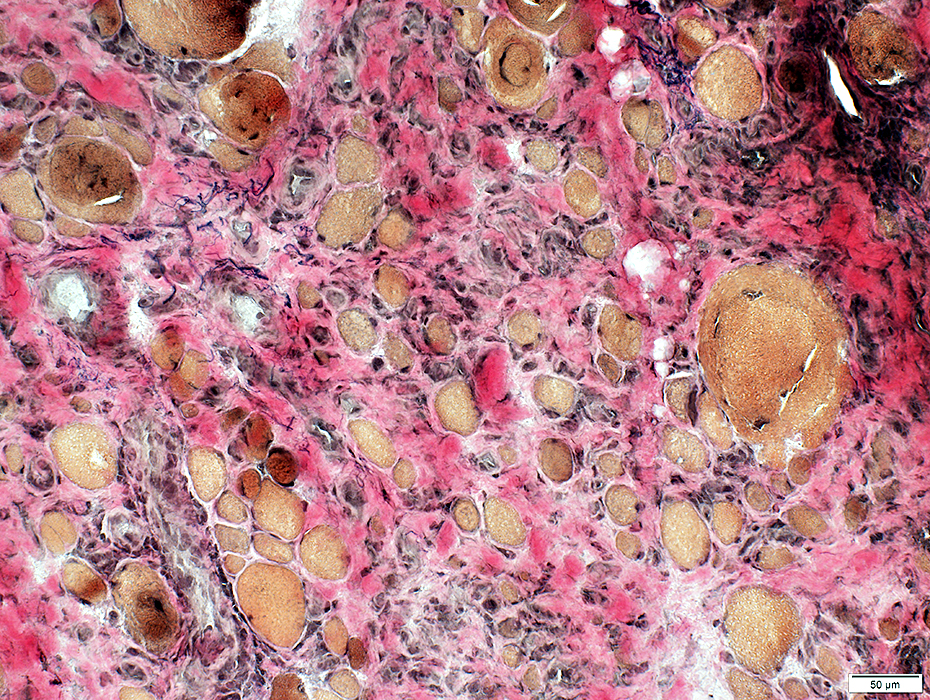 VvG stain |
 Gomori trichrome stain |
 ATPase pH 4.3 stain |
Type 2C on ATPase pH 4.3 stain
Cytoplasm stains for alkaline phosphatase
 Alkaline phosphatase stain |
Histiocytic (red stained) cells in endomysial connective tissue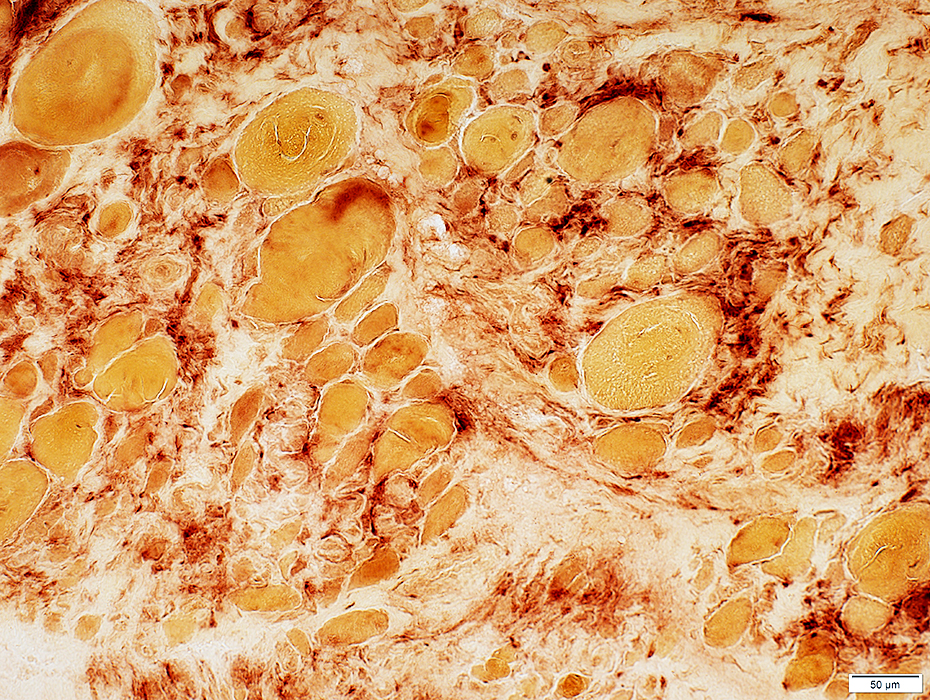 Acid phosphatase stain |
|
MHC Class I Normal on muscle fibers: No staining Present on endomysial cells 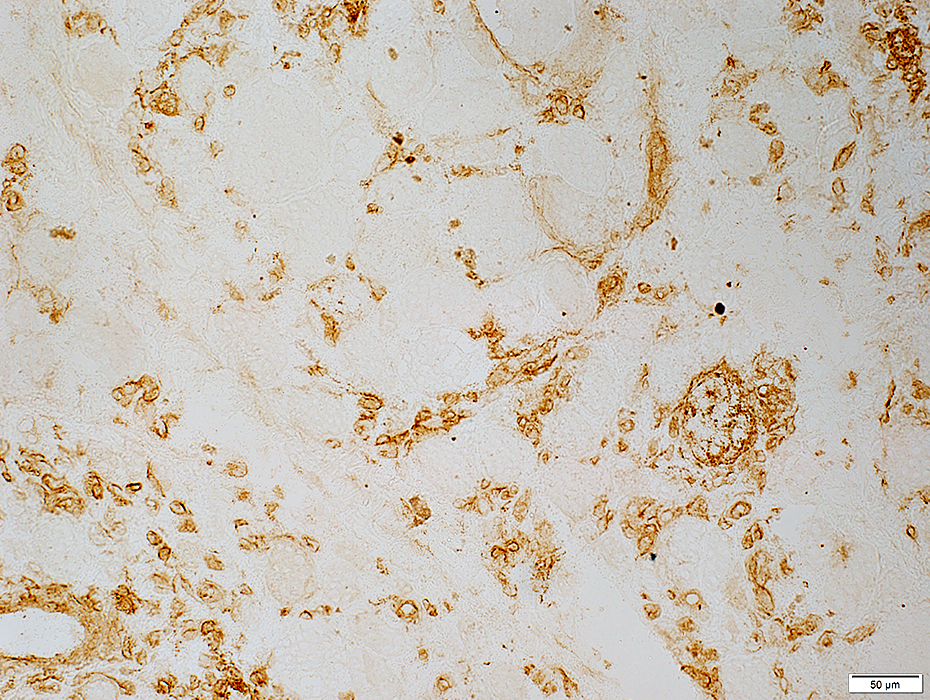 MHC Class I stain |
SRP Myopathy, Severe
Myofiber Basal Lamina Pathology
 Laminin-α2 stain |
 Laminin-α2 stain |
SRP: LATE, MILD PATHOLOGY, Months
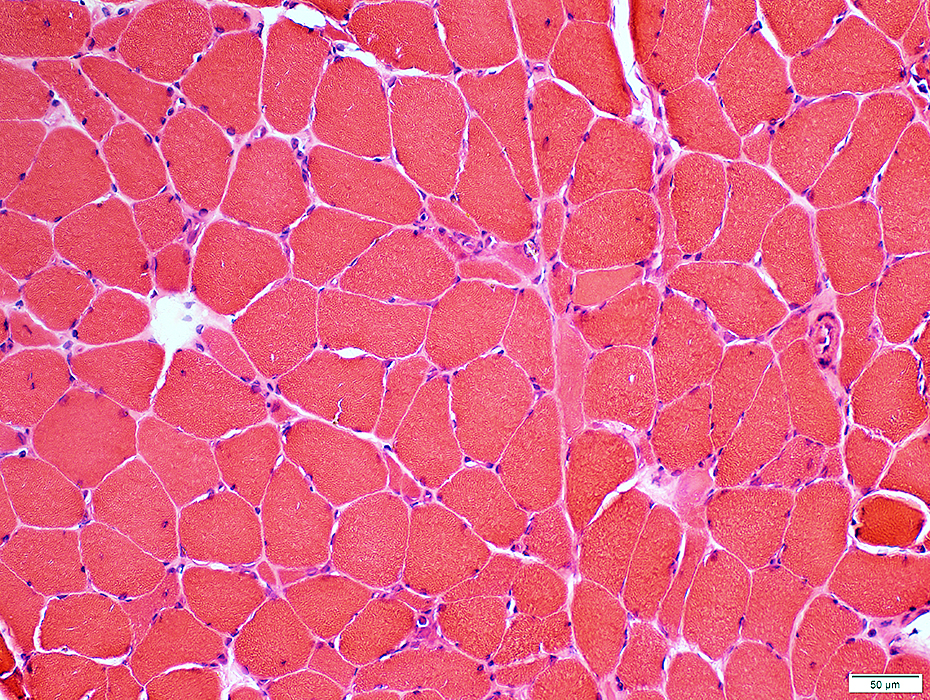 H&E stain |
Small muscle fibers: Angular; Basophilic cytoplasm
Endomysial connective tissue: Increased, Mild
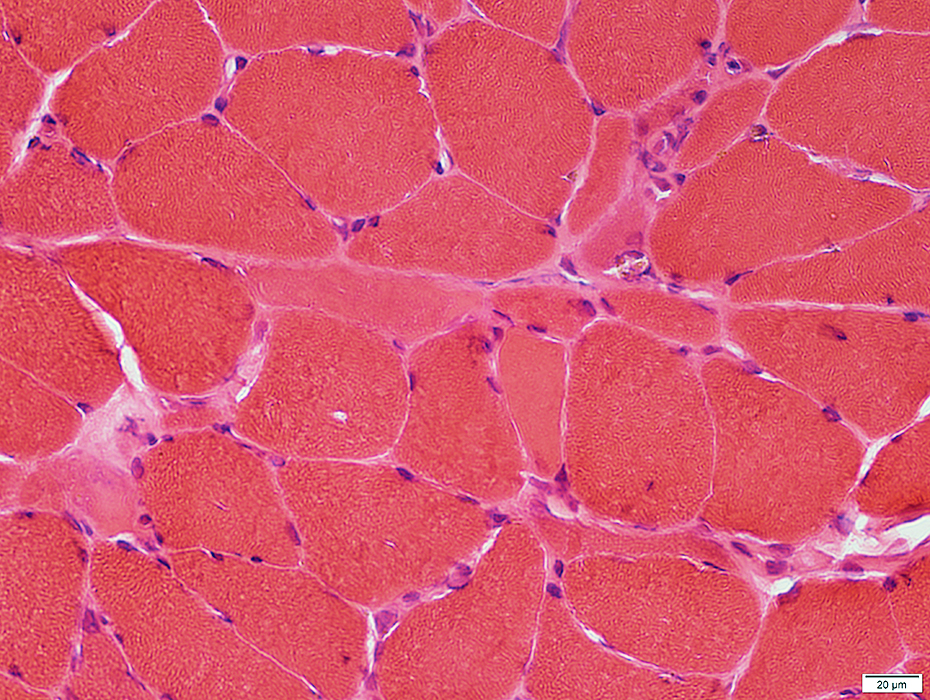 H&E stain |
 VvG stain |
Histiocytic cells: Scattered in endomysium
 Acid phosphatase stain |
 ATPase pH 4.3 stain |
Type 2C on ATPase pH 4.3 stain
Cytoplasm stains for alkaline phosphatase
 Alkaline phosphatase stain |
 C5b-9 stain |
MHC Class I: Not prominent on muscle fibers
 MHC Class I stain |
Neuromuscular junctions: Normal
 Esterase stain |
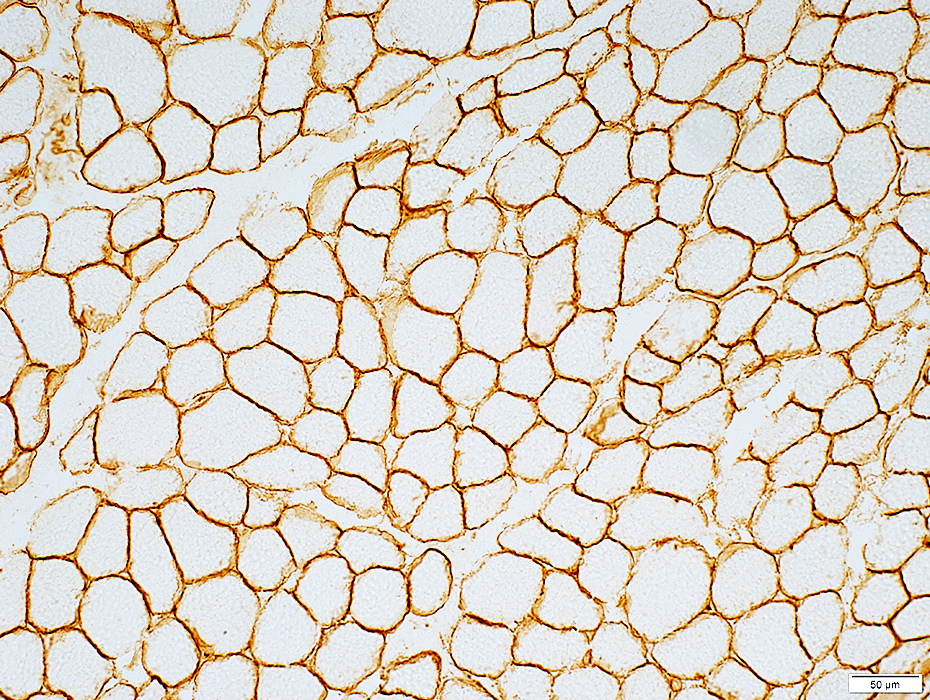
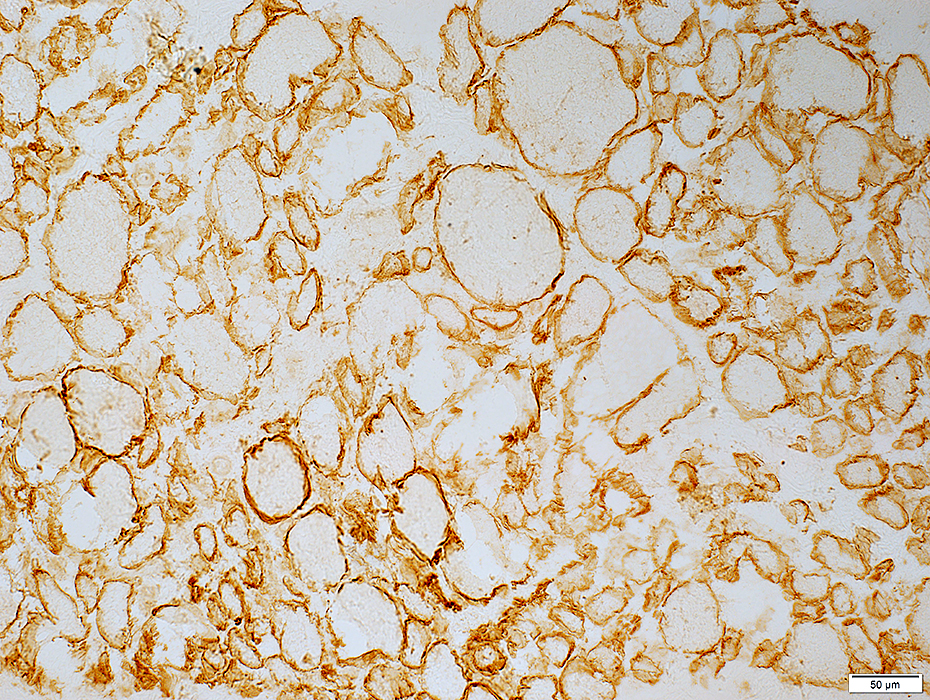
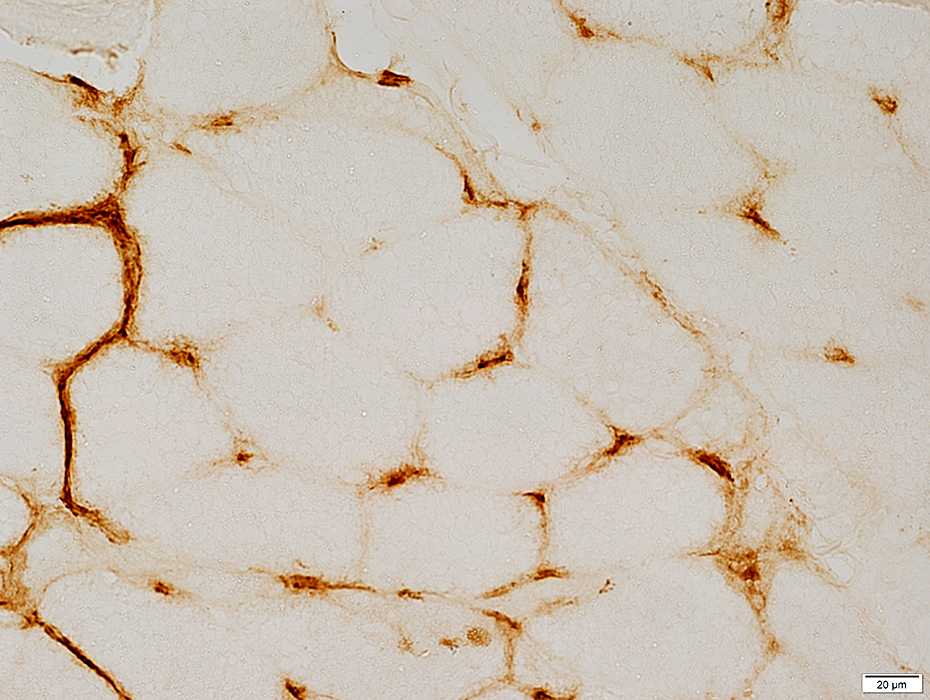
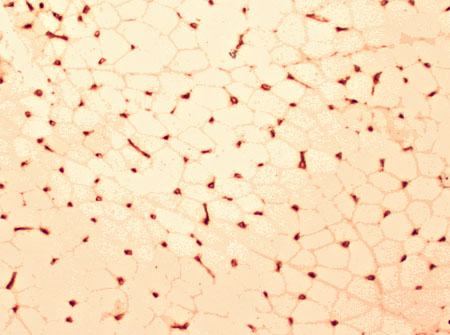
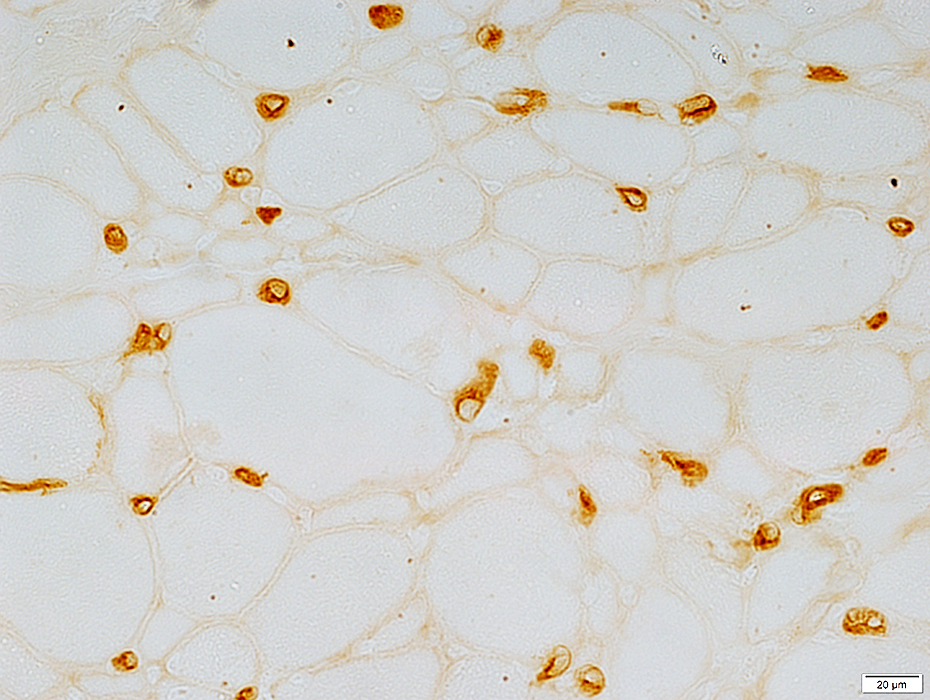
SRP MYOPATHY: CAPILLARY PATHOLOGY
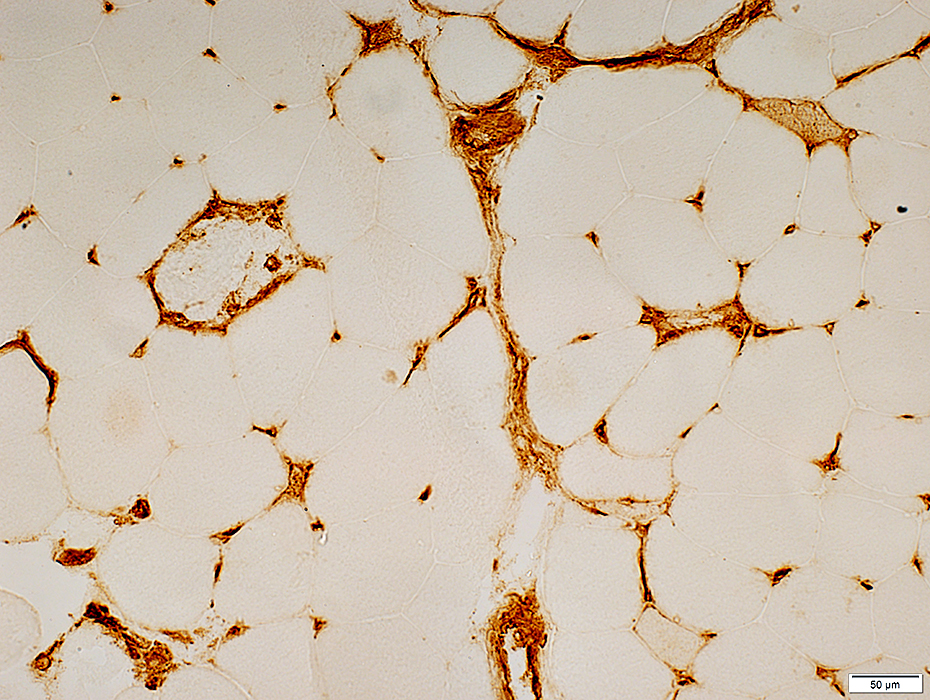
 Ulex europaeus agglutinin I stain SRP myopathy Endomysial capillaries: Large & Mildly reduced in number Some muscle fibers have no adjacent capillary |
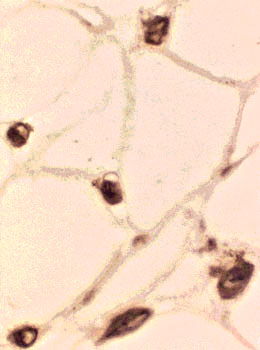 Ulex europaeus agglutinin I stain SRP myopathy Endomysial capillaries: Large |
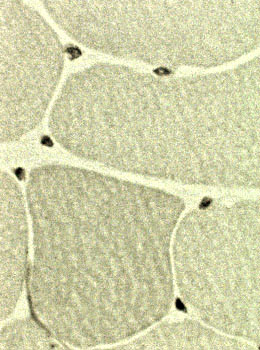 Ulex europaeus agglutinin I stain Normal muscle Endomysial capillaries: Small All fibers have adjacent capillaries |
 Ulex europaeus agglutinin I stain |
|
SRP MYOPATHY: MEMBRANE ATTACK COMPLEX (C5b-9) In cytoplasm of scattered necrotic muscle fiber On some capillaries | |
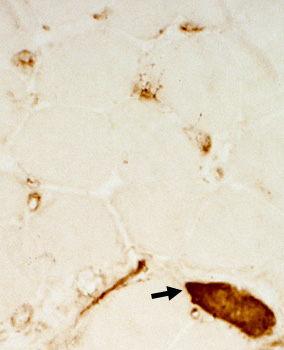 Antibody vs C5b-9 C5b-9 Deposition in endomysial capillaries and necrotic muscle fiber cytoplasm (Arrow) |
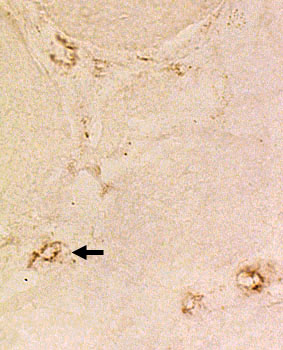
 Antibody vs C5b-9 C5b-9 Irregular deposition in endomysial capillaries (Arrows) |
Return to Inflammatory myopathies
Return to SRP myopathy
4/26/2023