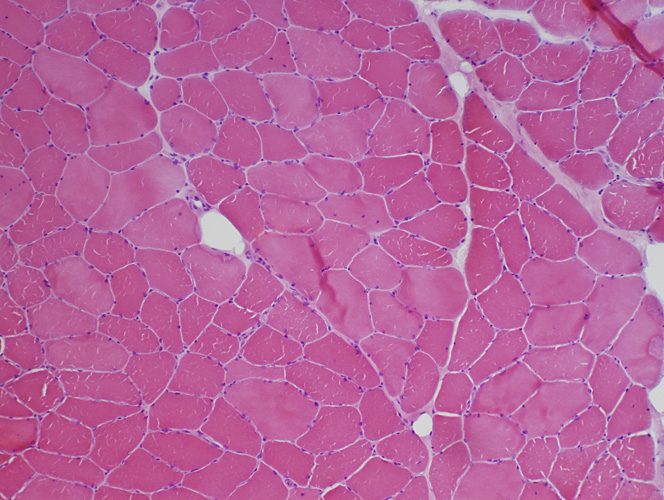
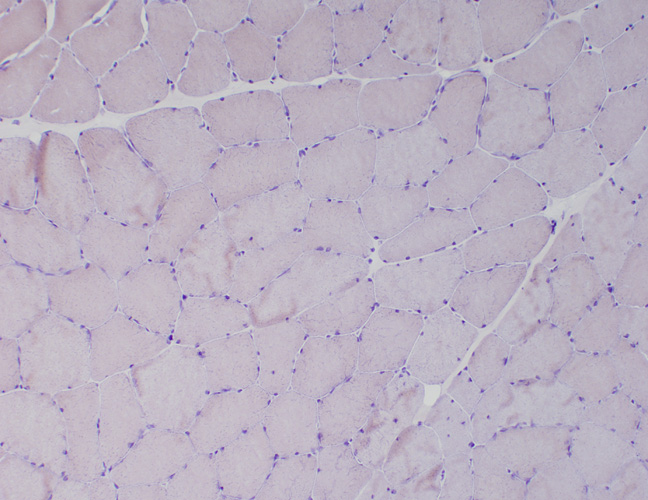
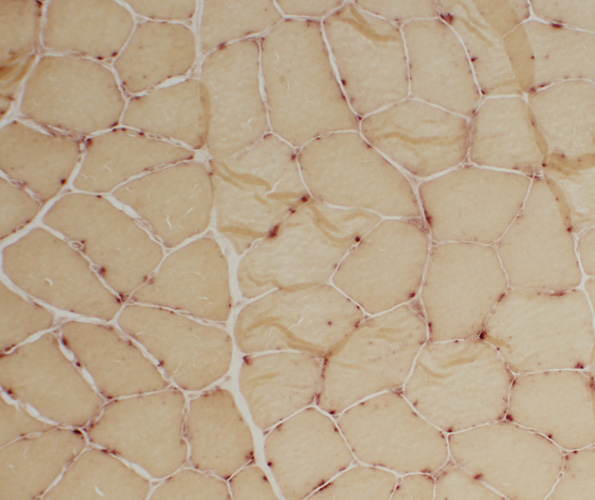
 H&E stain |
 Gomori Trichrome stain |
 VvG stain |
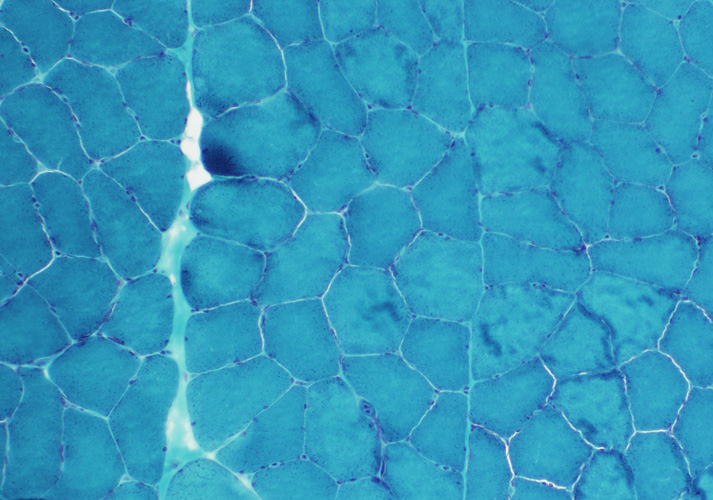
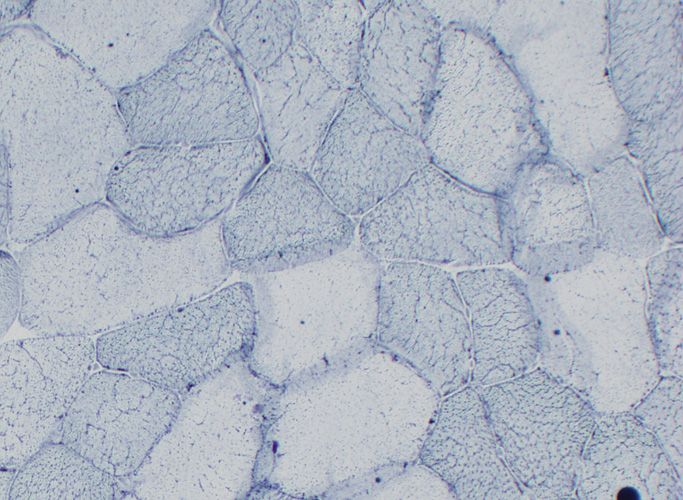
 NADH stain |
 Congo Red stain |
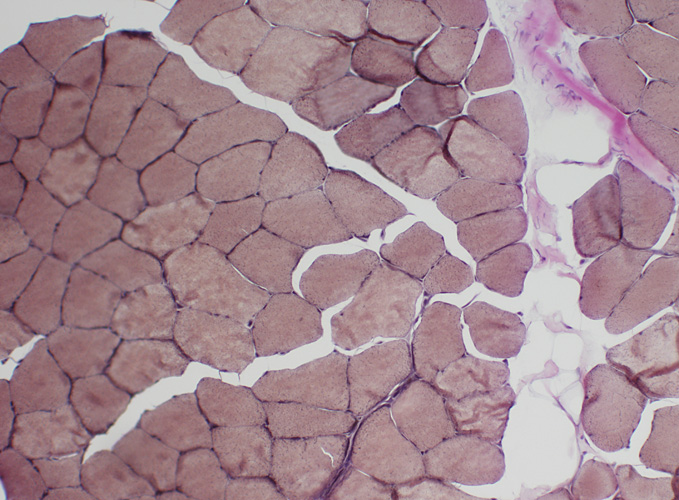
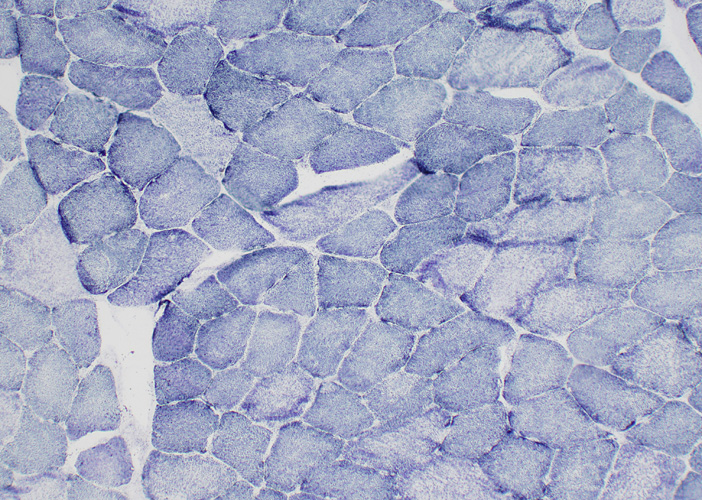
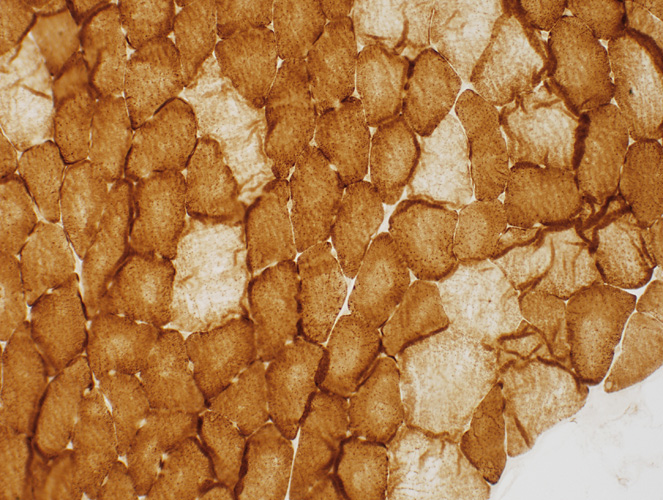
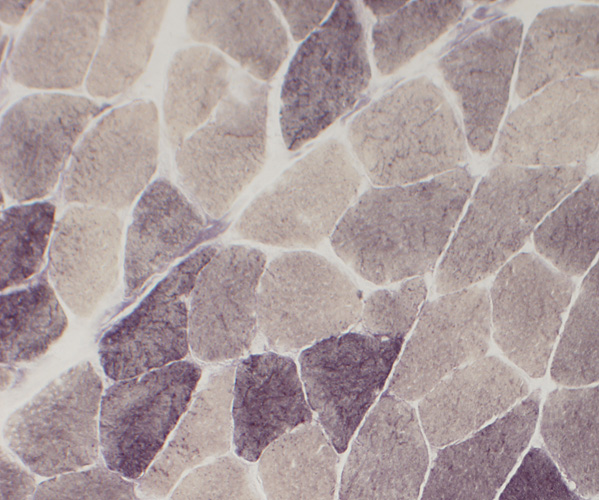
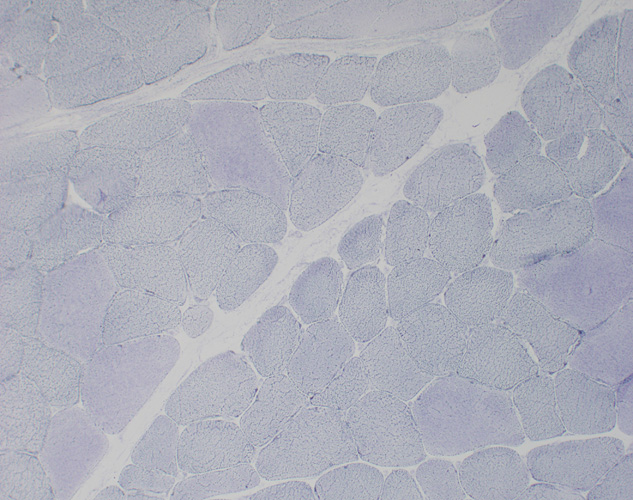
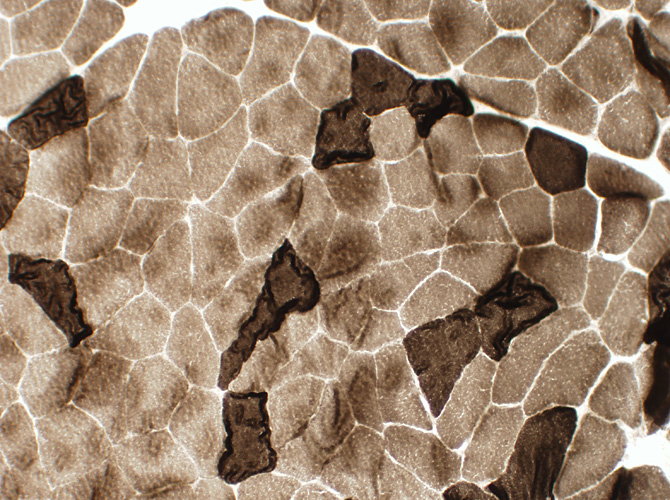 ATPase pH 9.4 stain |
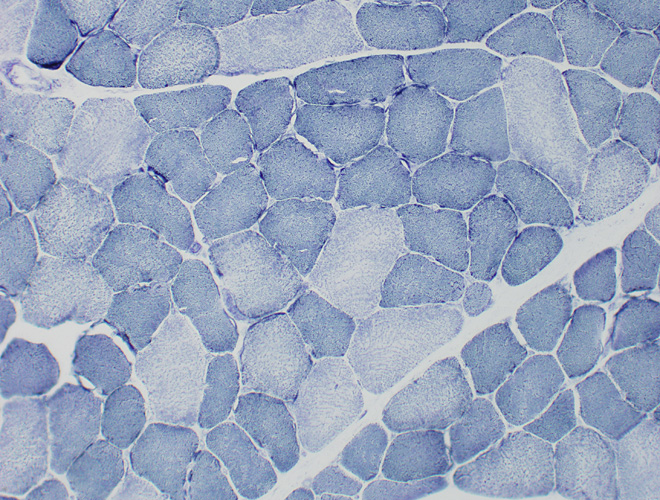
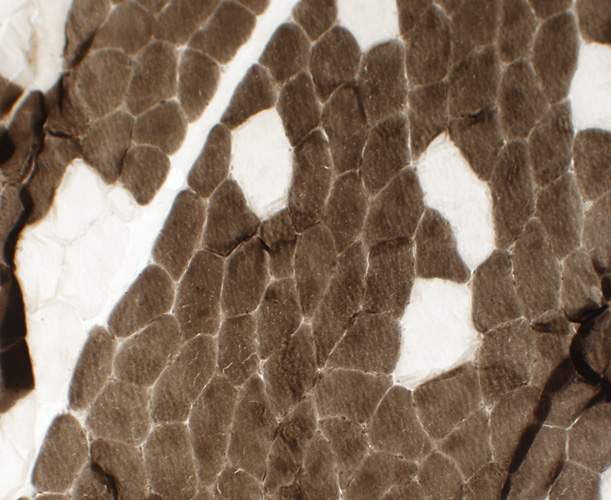 ATPase pH 4.3 stain |
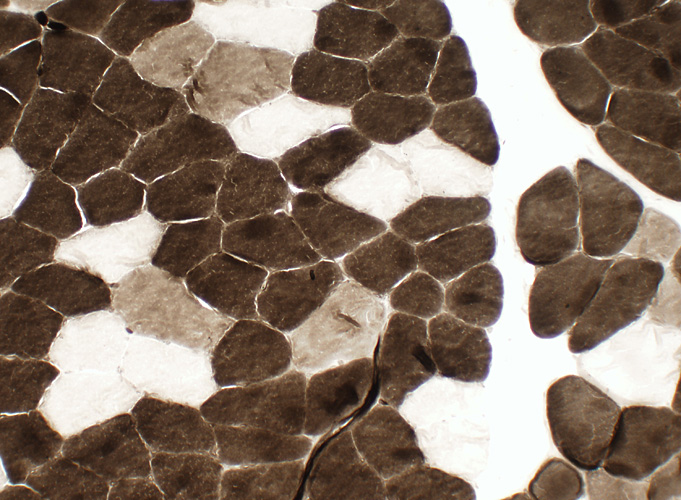 ATPase pH 4.6 stain |
 Alkaline Phosphatase stain |
 Acid Phosphatase stain |
 Esterase stain |
 Sudan Black stain |
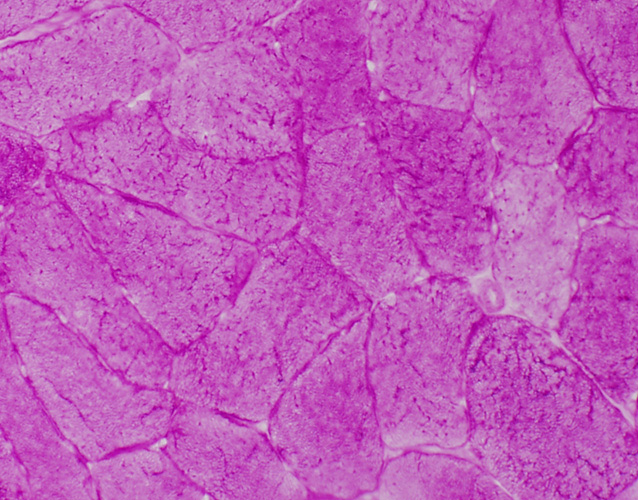 PAS stain |
 Succinate Dehydrogenase (SDH) stain |
 Cytochrome Oxidase (COX) stain |
 Phosphorylase stain |
 AMPDA stain |
|
BIOPSY REPORT Clinical history: 44-year-old male with pain Description of Muscle (Microscopic; Sections of snap frozen muscle): H&E stain shows mild variation in muscle fiber sizes with a rare smaller angular fiber. Endomysial connective tissue is normal. Vessels are normal. There is no mononuclear cell inflammation. There are no distinctive morphologic abnormalities on Gomori trichrome or VvG. Internal architecture is normal on NADH. There is no amyloid or inflammation on Congo red. ATPase (pH 9.4, 4.6 and 4.3) shows type I muscle fiber predominance. Type 1 muscle fibers are mildly smaller than type 2. There is a suggestion of fiber type grouping. Acid and alkaline phosphatase and Esterase are normal. SDH and COX are normal. There is no storage material on PAS or Sudan. AMPDA and phosphorylase are present. Interpretation: Non-diagnostic muscle biopsy. The minor fiber type grouping can suggest mild denervation and reinnervation. The mild degree of fiber type size disparity, with type 2 fibers larger than type 1, can be due to exercise. Type 1 muscle fiber predominance can be a normal finding in some muscles. It can also be seen with some chronic demyelinating neuropathies or with large fiber type grouping. |