CENTRAL CORE DISEASE: Pathology
|
General description Adult Child DDx Myopathy Morphology Ultrastructure |
|
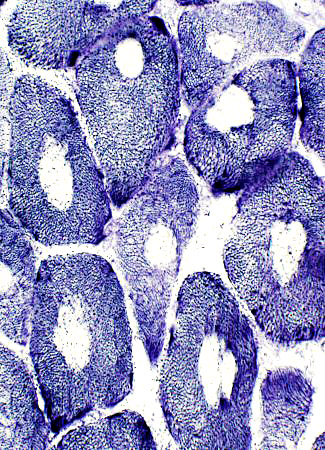
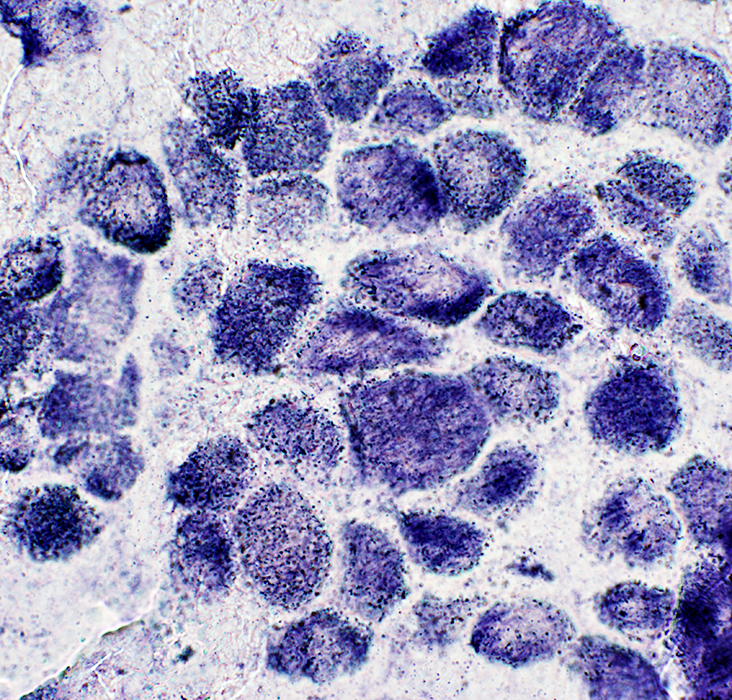
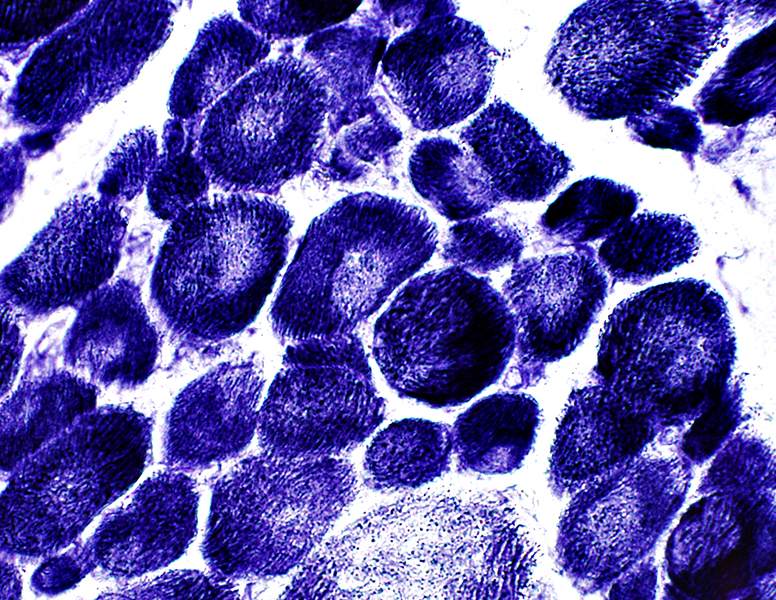
 NADH stain |
|
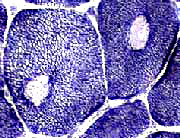
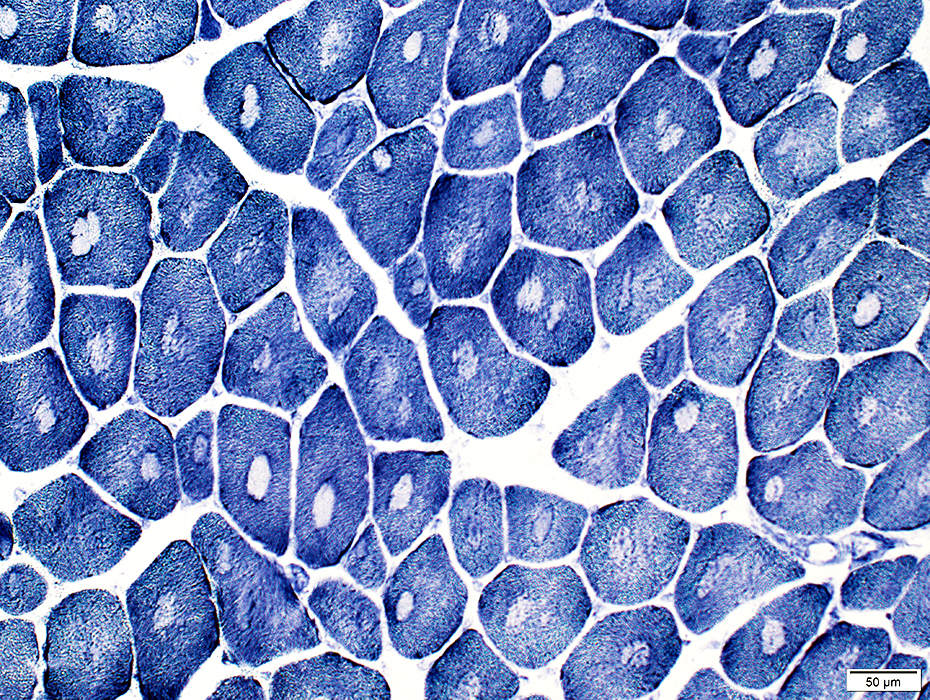
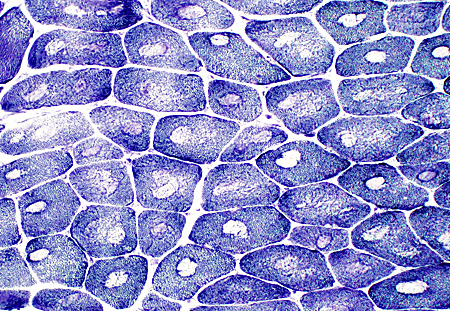
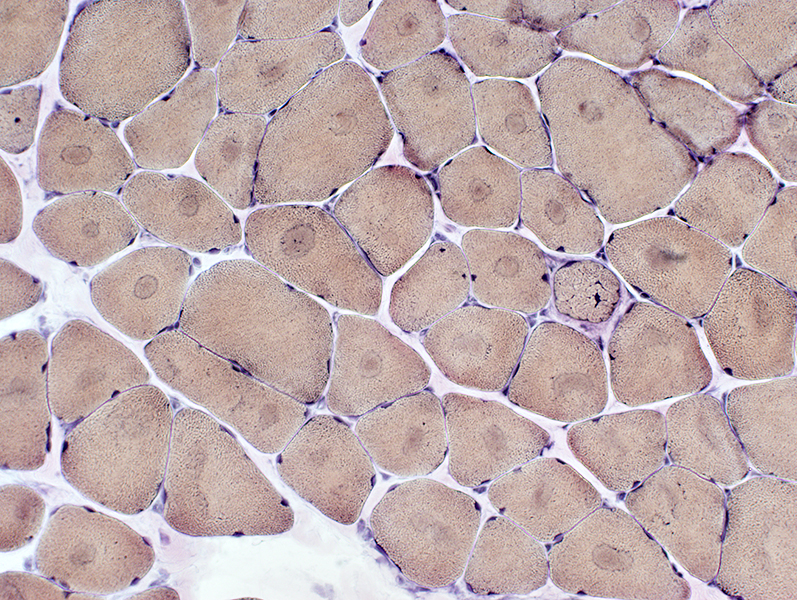
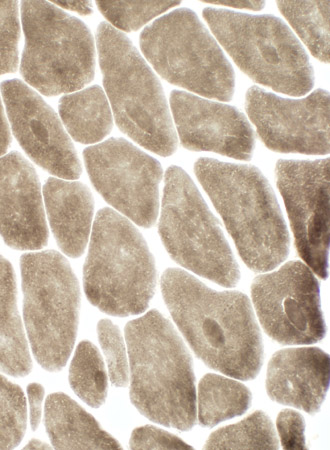
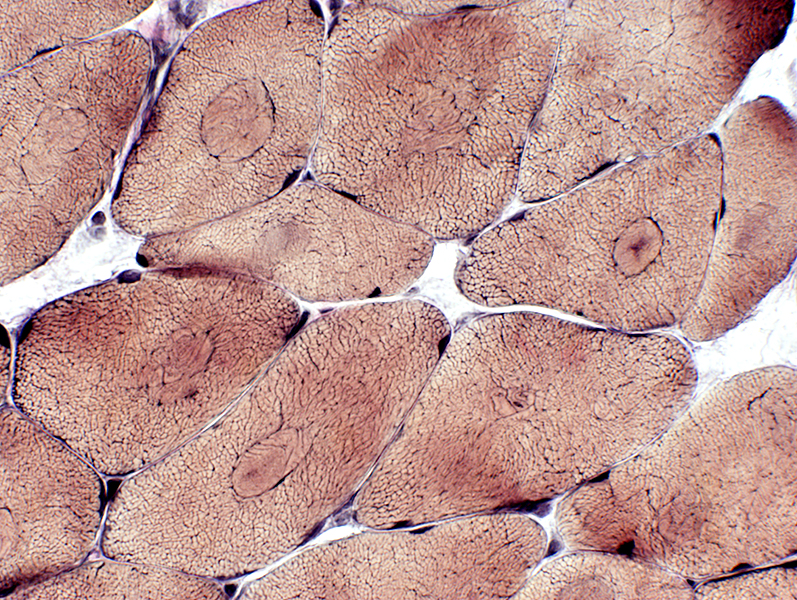
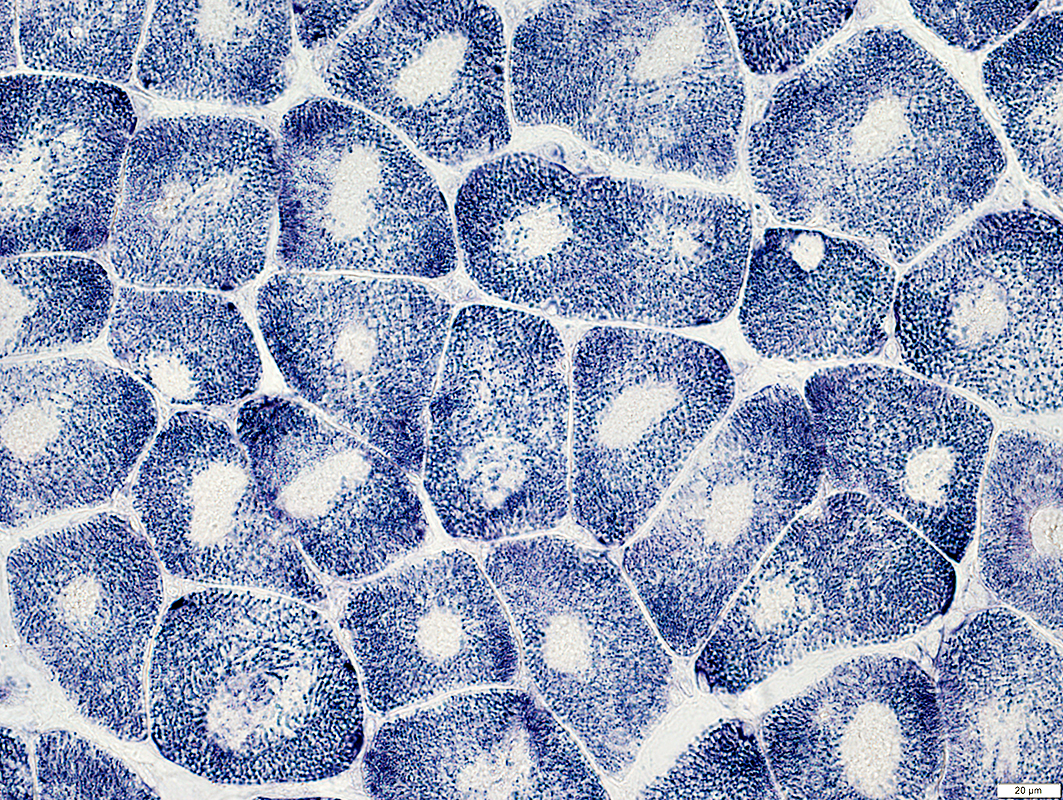
Cores Central clear zone in fibers stained for cytoplasmic or mitochondrial membranes NADH stain: Well defined central region of reduced staining Cores run whole length of muscle fibers 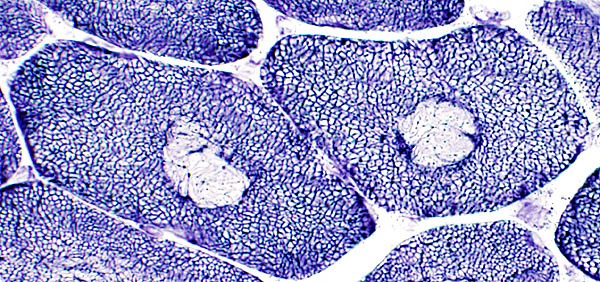
|
 NADH stain |
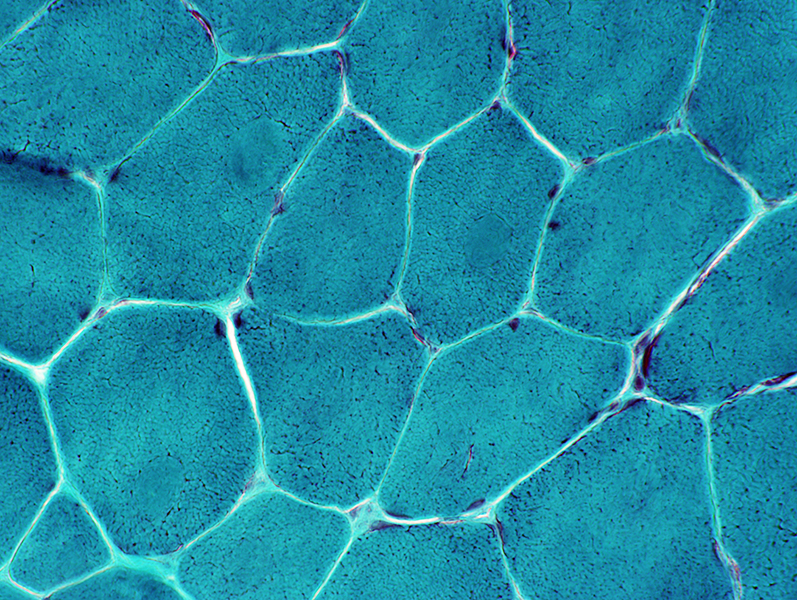
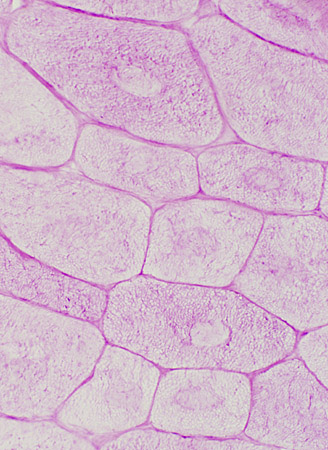
 VvG stain Cores are visualized well with VvG but not H&E stain |
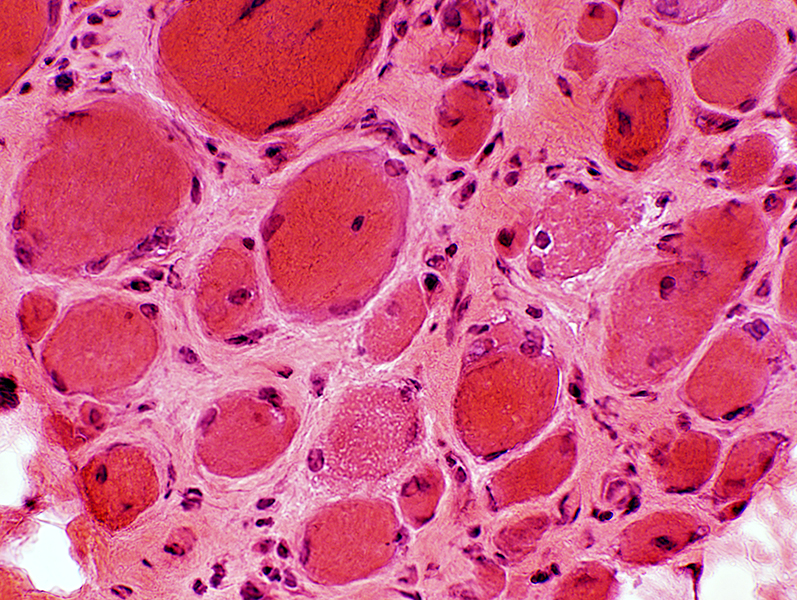
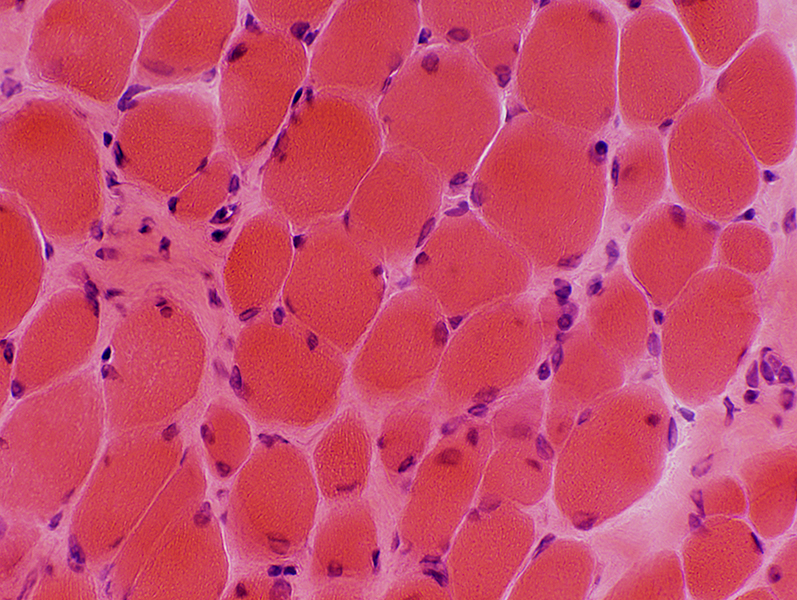
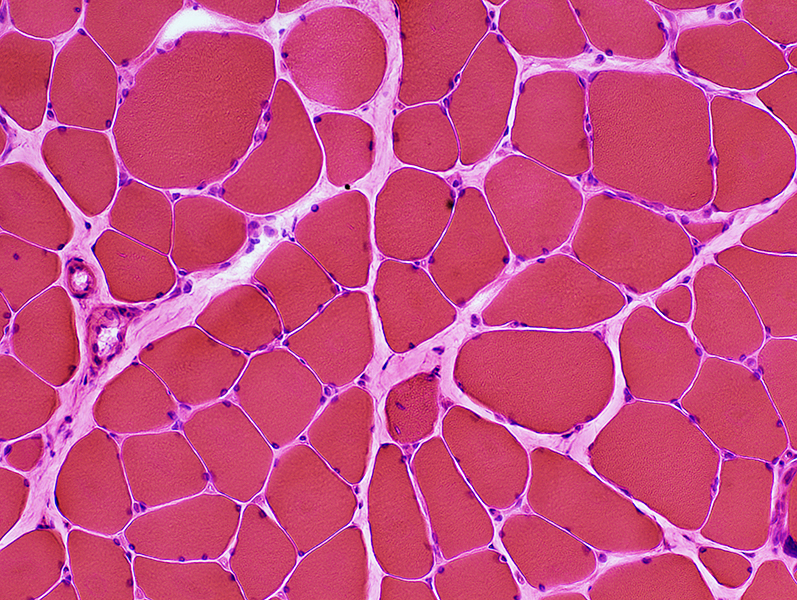 H&E stain |
Central Core Disease: Adult
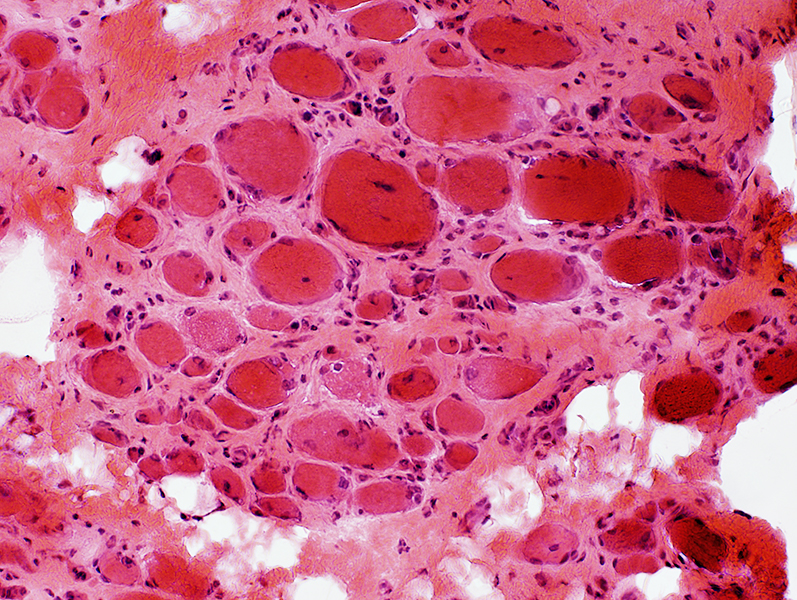
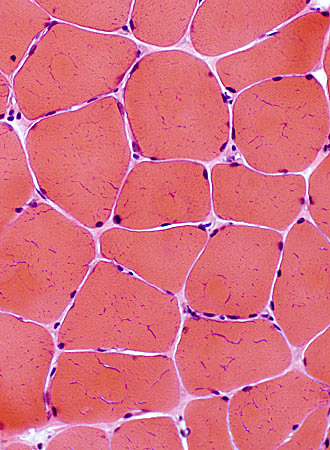 H&E stain |
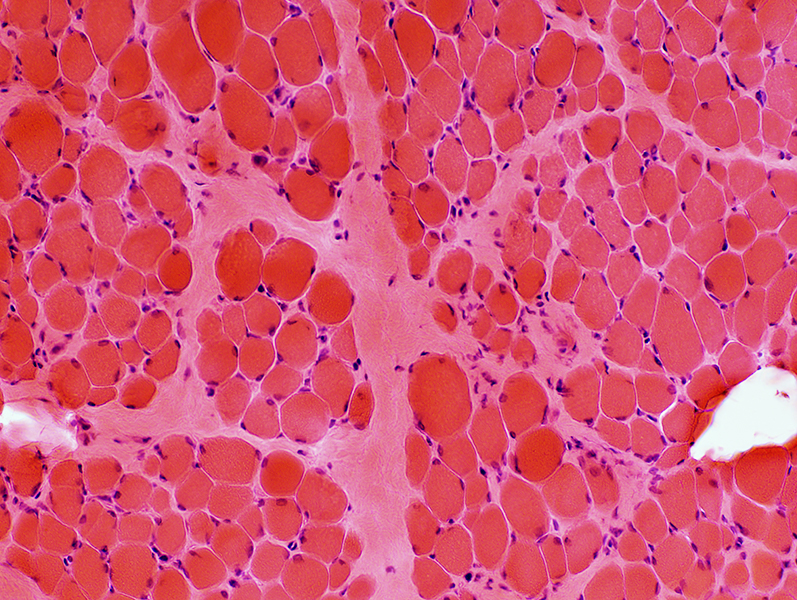
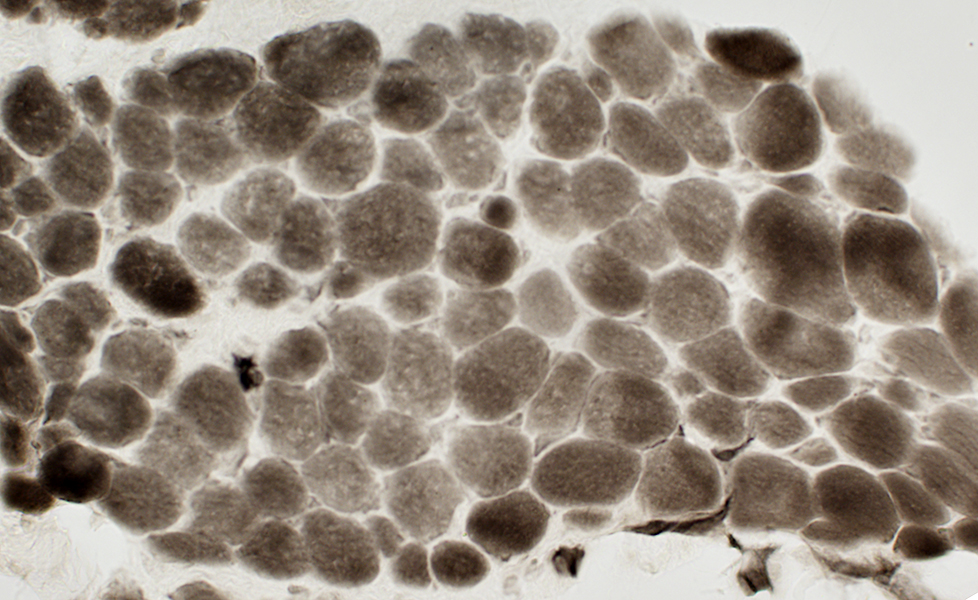
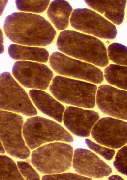 ATPase, pH 9.4 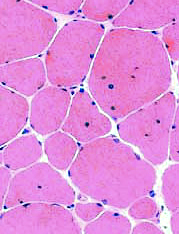 H&E stain |
 ATPase, pH 9.4 |
Fiber size: Variability
Connective tissue: Normal or Mildly increased
Internal nuclei: Some muscle fibers
Muscle fiber types
Marked type I muscle fiber predominence
Some cores have loss of central myofibrillar structure
 NADH stain |
Cores are rounded & have sharply delineated borders
Some muscle fibers have irregular centers, but not well formed cores
 NADH stain |
 VvG Some cores are visible on VvG or Gomori trichrome stains |
 Gomori trichrome |
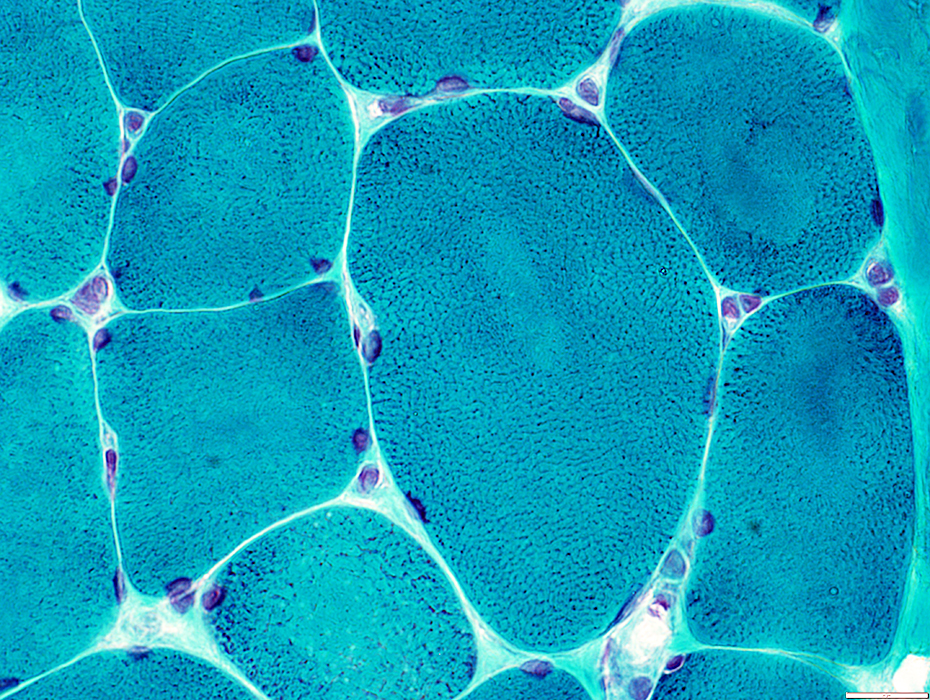 Gomori trichrome |
|
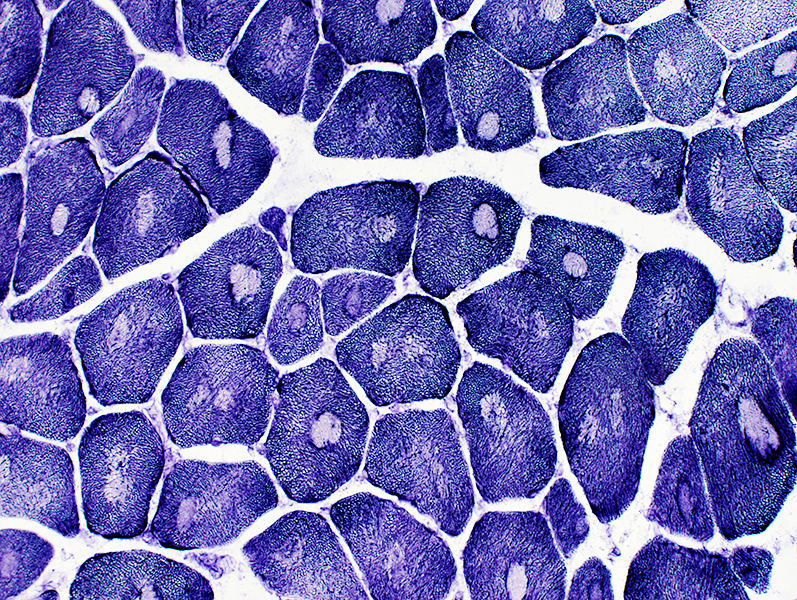
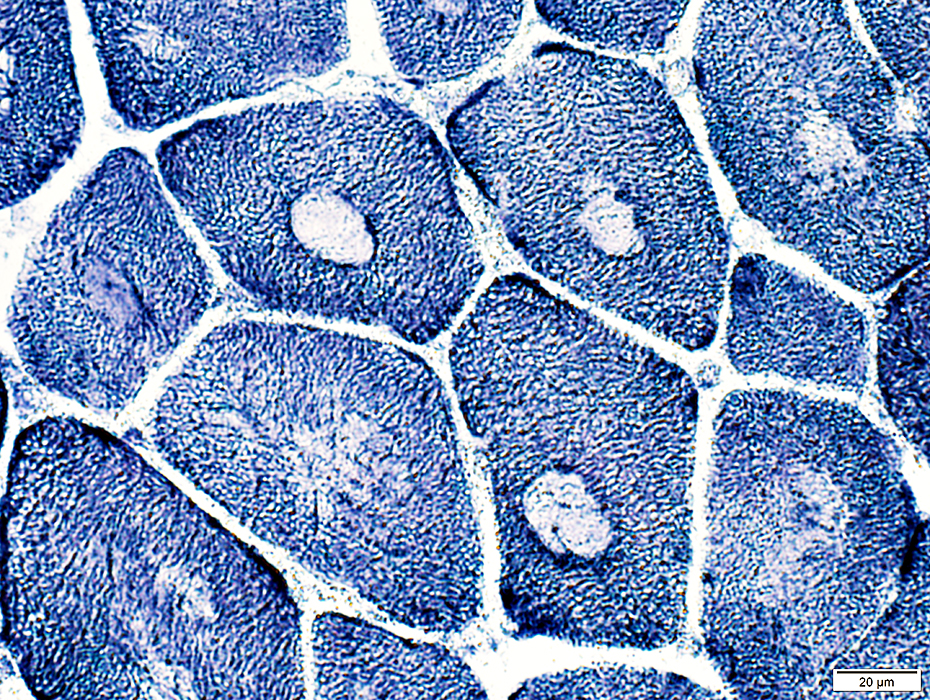
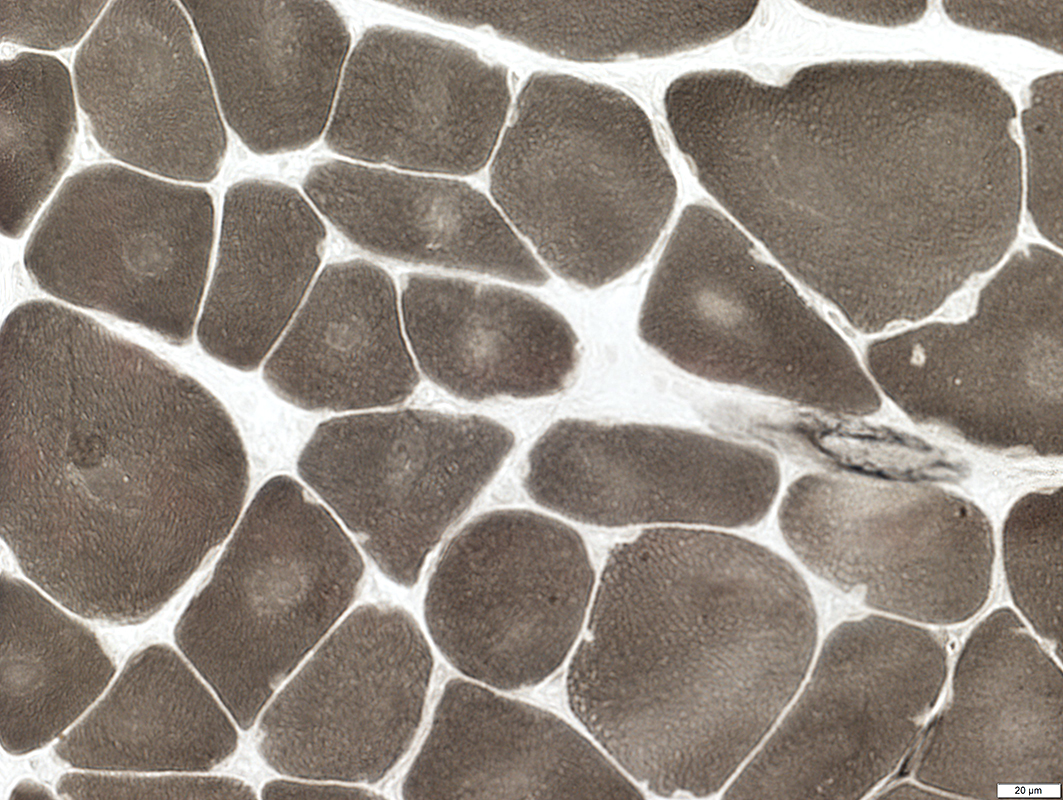
All fibers are Type I: Central cores are visible 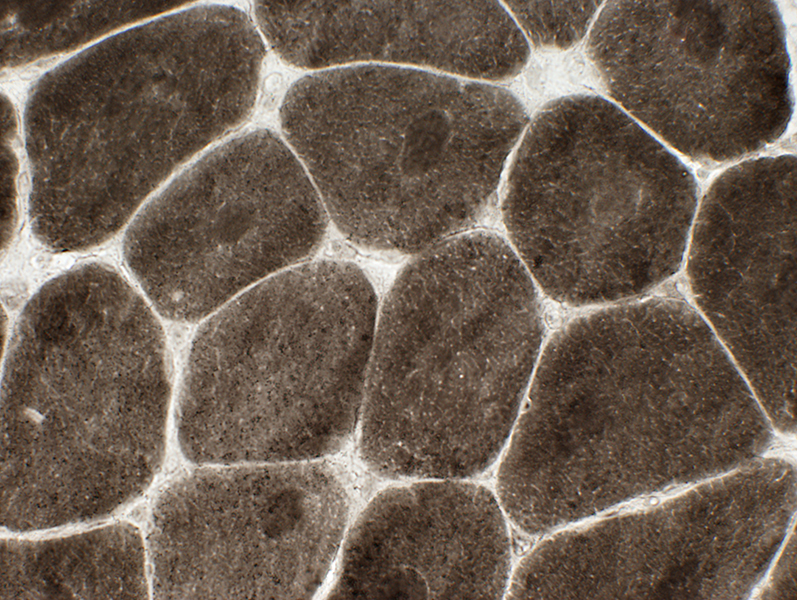 ATPase, pH 9.4 |
 SDH stain |
 PAS stain |
|
Mitochondria Not present in cores |
Glycogen Variably present in cores |
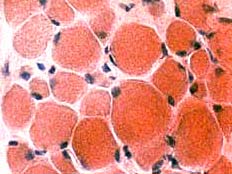
Actin: Increased within central cores
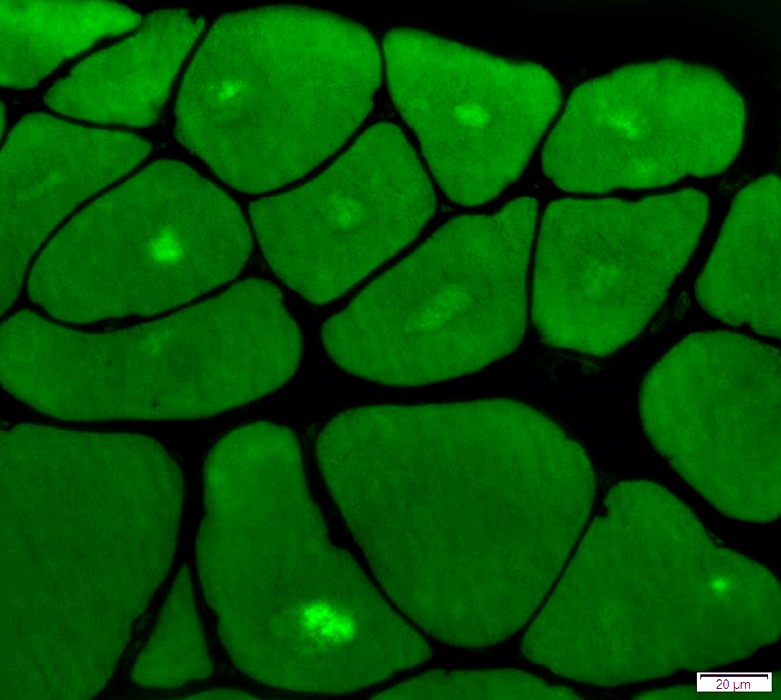 Phalloidin stain |
Central Core Disease with Myopathy
 H&E stain |
 H&E stain |
 NADH stain |
Central Core Disease: Young Child
 H&E stain |
 H&E stain |
 H&E stain |
 Gomori trichrome stain |
 NADH stain |
 ATPase pH 9.4 stain |
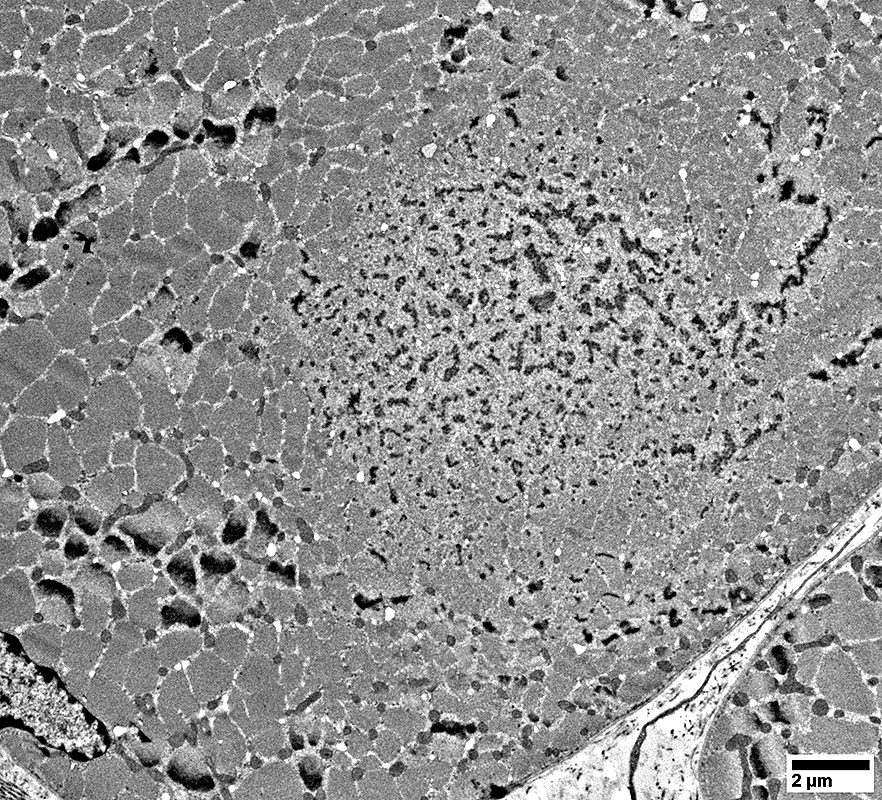
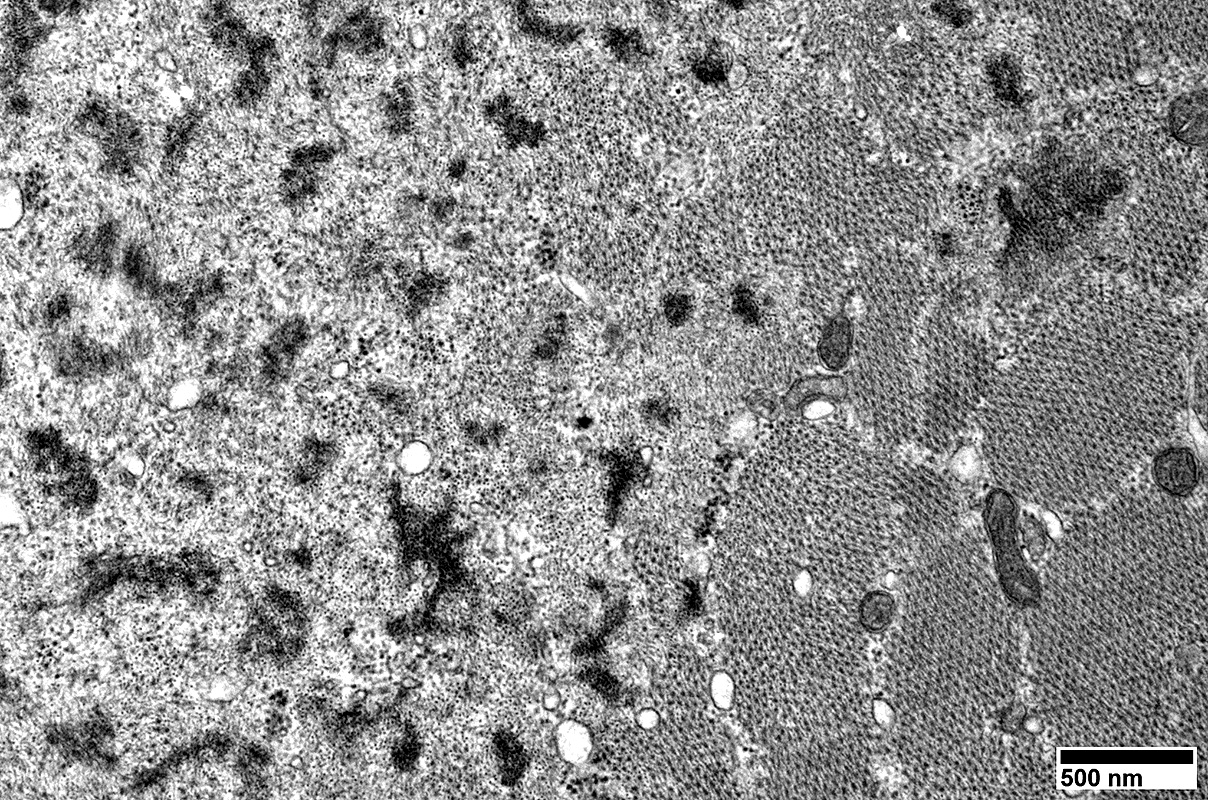
Cores: Ultrastructure
Focal Myofilament DisruptionExtends along most of length of muscle fiber
Often stain for: Actin; α-Actinin; Desmin; αB-crystallin
|
|
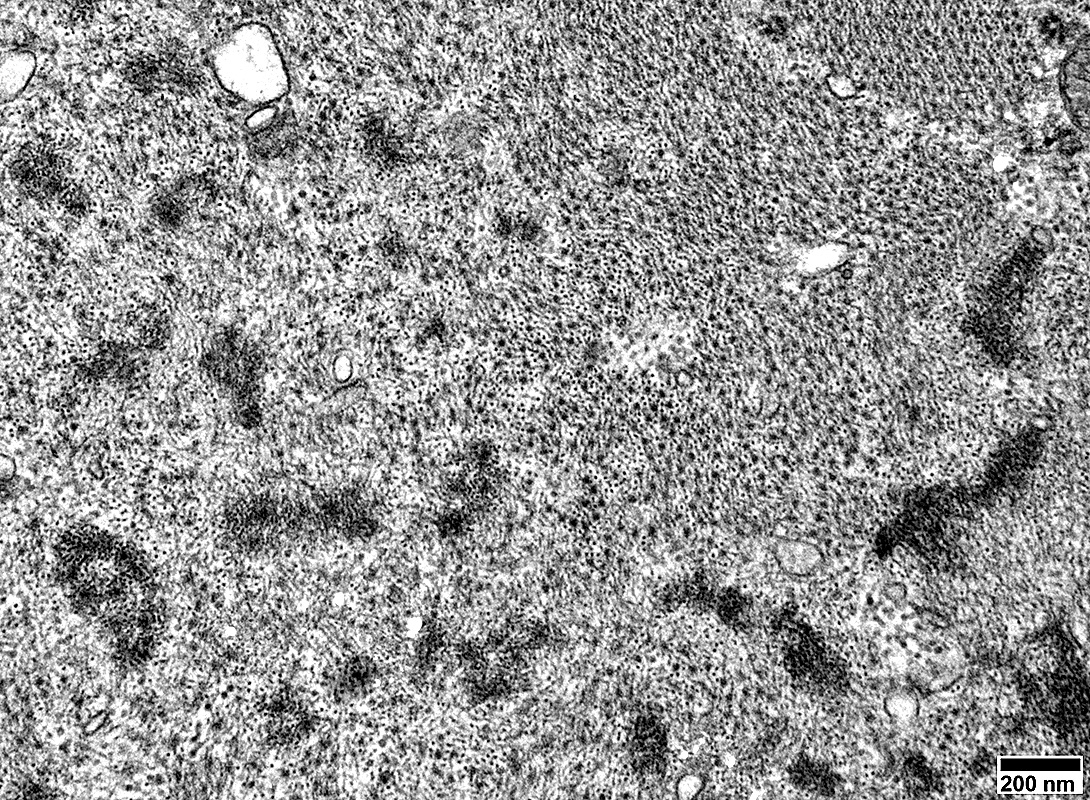
Myofibrils: Disrupted organization
Foci of loss of myofilaments
No mitochondria
|
|
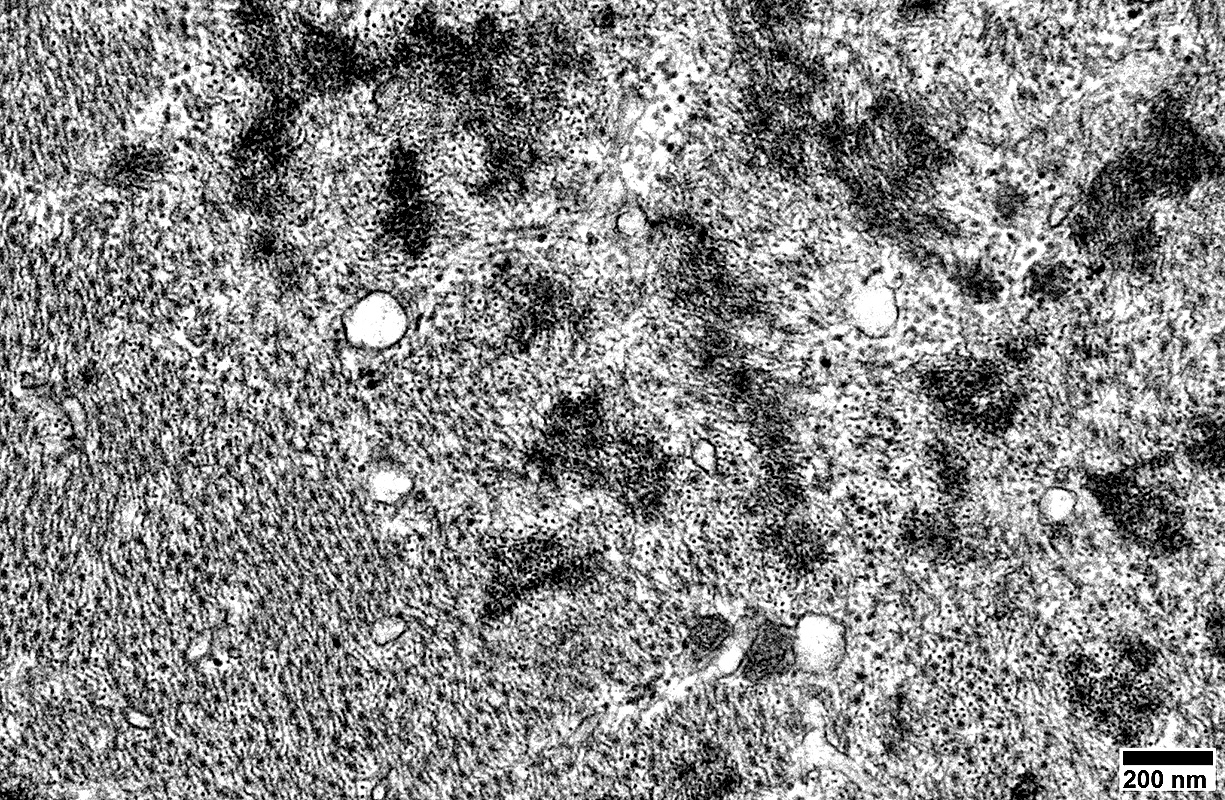
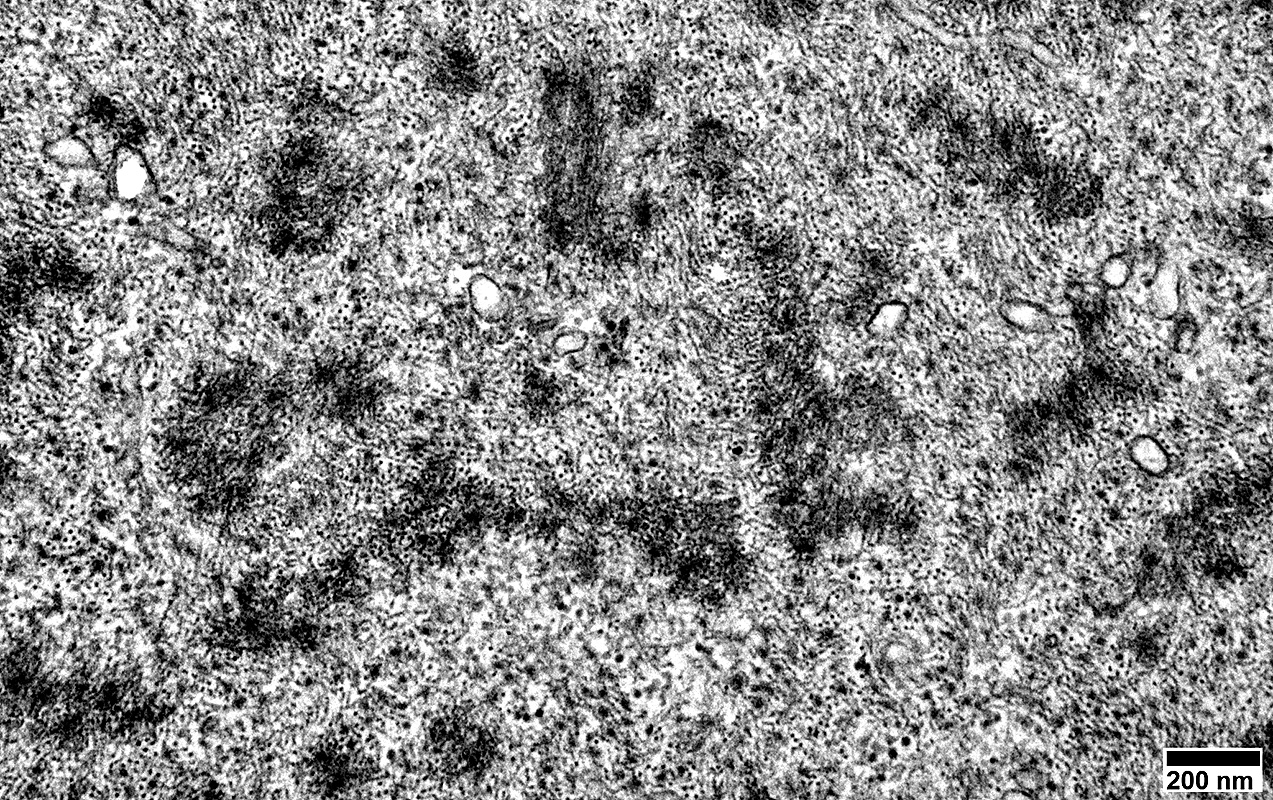
Myofibril organization: Disrupted
Myofilament loss
Mitochondria: Absent
Z-band material: Excess
|
Histology of Central Cores in this muscle
Cores (Round, Central clear regions) in most muscle fibers
 NADH stain |
Cores are visible in some fibers
 ATPase pH 9.4 stain |
Return to Congenital myopathies
Return to Neuromuscular Home Page
3/11/2020